Results for “plasma” 42 found
Convalescent plasma?
Here is the FDA press release. Here is StatNews coverage. Scott Gottlieb tweets:
The available data seems to meet the bar for an EUA.
Here is his WSJ Op-Ed with McClellan, Straussian throughout I suspect. They will only hint at their outrage at the process, noting that both are former FDA heads. Here is the FDA truth twist.
I found this Adam Rogers Wired piece insightful and the best single treatment so far, and also interesting more generally on RCTs:
“Fifty thousand people have been given a treatment, and we cannot know whether it worked or not,” says Martin Landray, one of the leaders of the Randomised Evaluation of Covid-19 Therapies (or Recovery) Trial in England, a large-scale, multi-center, multi-drug randomized controlled trial that showed that the corticosteroid dexamethasone saved the lives of Covid-19 patients and the autoimmune drug hydroxychloroquine did not. (That 50,000 number was from a few weeks back, just after the plasma preprint came out.)
The main arguments against the decision from Trump/FDA seem to be “do RCTs” and “convalescent plasma isn’t shown to be so great.” But those points have it exactly backwards. Patients for trials are extremely scarce right now, and if convalescent plasma is not the highest probability big winner (and I suspect it isn’t), you won’t want to waste scarce patients on doing the RCT. Moreover, if you can’t get the RCT done with 98,000 or so patients, maybe you’re just not up to doing it period! (Please do think at the margin.) In the meantime, convalescent plasma does not seem to involve harms or risks, and it may offer some benefits. So why not let more people have easier access to it?
And might there be a tiny chance that American citizens demand stronger payment incentives for the relevant supplies here and also for other treatments?
If all people have is “do RCTs and CP isn’t shown to be so great,” I don’t think they have begun to engage with the arguments. And additionally politicizing the FDA is definitely a real cost to be reckoned with, but the Twitter noise I am seeing from public health experts seems oblivious to the fact that the FDA’s ex ante risk-averse stance was politicized to begin with (which is not necessarily a bad thing, but yes this is a basic fact — “politicization for me, but not for thee,” etc.).
Alex Armlovich on blood plasma donors and markets
From my email:
I saw your post about COVID blood brokers–My girlfriend and I had it in March and finally got antibody tests last week when the city opened the free clinics.
I inquired on a national plasma donor site, was directed to CSL Plasma in Clifton NJ, and a donor concierge from LeapCure reached out. They didn’t tell me what the compensation is (the CSL website says it’s usually ~$50 for normal plasma) but they’re calling a roundtrip Uber from my apartment near Ridgewood, Queens all the way to NJ, which is $108 one-way. The concierge said to reach out if there are any concerns with the first trip next week because they’re hoping for up to 2x weekly donations.
What I don’t understand is, why doesn’t the city’s antibody testing program directly link up to plasma donation? I had to go through a bunch of hassle to find out where to donate, and I think the information & coordination friction is a bigger deterrent than anything else. And why isn’t there more collection capacity in the city itself; the long commute seems unnecessary. If this is scientifically important enough to merit real donor spending from biotech, it seems like the city should make even a minimal investment in reducing process friction.
Maybe an integrated, frictionless testing & plasma donation infrastructure should be a permanent strategy for future “zero-day viruses” where convalescent antibodies are the only thing we have to treat first responders…
Here is Alex Armlovich on Twitter.
Incentivizing Plasma Donation for Convalescent Therapy
Kominers, Pathak, Sonmez, and Unver apply market design tools to incentivize convalescent therapy:
COVID-19 convalescent plasma (CCP) therapy is currently a leading treatment for COVID-19. At present, there is a shortage of CCP relative to demand. We develop and analyze a model of centralized CCP allocation that incorporates both donation and distribution. In order to increase CCP supply, we introduce a mechanism that utilizes two incentive schemes, respectively based on principles of “paying it backward” and “paying it forward.” Under the first scheme, CCP donors obtain treatment vouchers that can be transferred to patients of their choosing. Under the latter scheme, patients obtain priority for CCP therapy in exchange for a future pledge to donate CCP if possible. We show that in steady-state, both principles generally increase overall treatment rates for all patients|not just those who are voucher-prioritized or pledged to donate. Our results also hold under certain conditions if a fraction of CCP is reserved for patients who participate in clinical trials. Finally, we examine the implications of pooling blood types on the efficiency and equity of CCP distribution.
The idea is quite similar to the “no give, no take” rule for organ donation that I have promoted for many years. Namely, if you don’t sign your organ donor card you go to the back of the queue should you ever need an organ donation. Israel adopted the idea some years ago by giving points to people who signed their organ donor card. As with no-give, no-take, the point of the rules that Kominers et al. promote isn’t fairness per se but rather as an incentive to increase donations and thus increase the supply of plasma.
Dear Canada: Don’t Ban Paid Blood Plasma Donation
The United States has been called the OPEC of blood plasma because it exports hundreds of millions of dollars worth to other countries. Why does the US dominate the blood plasma industry? Because in the U.S. it’s legal to pay donors which increases supply. Some provinces in Canada have also allowed paid donors but 80% of the blood plasma given to Canadians is imported from the United States and, to make matters worse, some provinces have banned or are considering banning paid donation. A very good letter opposes the ban:
We are professional ethicists in the fields of medical ethics, business ethics, and/or normative ethics, and academic economists who study how incentives and other mechanisms affect individual behaviour. We all share the goal of improving social welfare.
We have strong reservations regarding any Act or legislation (hereafter: “Acts”) that would prohibit compensation for blood plasma donations…….Both the ethical and the economic arguments against a compensatory model for blood plasma for further manufacture into PDMPs are weak. Moreover, significant ethical considerations speak in favour of the compensatory model, and therefore against the Acts.
The letter carefully discusses many of the objections such as that paid donations will drive out unpaid:
The compensatory model leaves open the possibility of donors’ opting out of compensation, or the operation of a parallel non-compensatory model. The United States does just this, and has an approximately 50% higher voluntary, unpaid, per capita blood donation rate than Canada. Germany, Austria, and the Czech Republic, where plasma donors can be compensated, likewise all have higher rates of voluntary, unpaid per capita blood donation than Canada.
Is paid blood plasma less safe?
Dr. Graham Sher, the CEO of Canadian Blood Services, has said, “It is categorically untrue to say, in 2015 or 2016, that plasma-protein products from paid donors are less safe or unsafe. They are not. They are as safe as the products that are manufactured from our unremunerated or unpaid donors.”
The letter is signed by two Nobel Prize winners in economics, Alvin Roth and Vernon Smith, by philosophers like Peter Jaworski, who did most of the heavy lifting, and by experts who have studied incentives and blood donation closely like Nicola Lacetera and Mario Macis. I am also a signatory.
EU May Ban Payments for Milk, Sperm and Blood
BrusselsSignal: The European Parliament has approved a draft regulation banning payments for breast milk, sperm, blood and other “substances of human origin” (SoHO).
Billed as an attempt to increase safety across the bloc, the ban allegedly aims to ensure that those who are financially disadvantaged within the bloc are not subject to undue pressure to donate their cells and bodily fluids.
Hmmm. Why not ban the sale of labor to protect financially disadvantaged labor donors from undue pressure? Indeed, why not require that dangerous jobs like mining pay low wages so we can be sure that no one is induced to do these jobs by financial pressure?
More prosaically, the European Union falls short of producing all the blood plasma it needs to meet its demand for life-saving medicine. Consequently, the European Union depends on imports—primarily from compensated donors in the United States—to address its plasma deficit. Should the proposed EU legislation be enacted, the deficit is likely to get worse because Germany, Austria, Hungary, and the Czech Republic, currently permit financial compensation. Indeed the U.S. and these EU countries together account for 90% of the global plasma supply. A ban on paid donations within the EU will thus decrease the quantity of plasma supplied from Germany, Austria, Hungary, and the Czech Republic and force the EU to rely even more on imports from the US.
The US is also the world’s biggest exporter of human sperm because US sperm donors can be compensated and remain anonymous (depending on the state). US donors are also carefully screened for quality, in part due to US regulations and in part due to market demand for information about the donors. Denmark is also a major exporter of sperm, in part because it, too, allows financial incentives to donors. Reduced donations from Denmark will make the European Union increasingly dependent on U.S. sperm supplies. Indeed, after Canada banned paid sperm donors in 2004, the supply of Canadian donors plummeted to just 35 (!) and US sperm exports to Canada increased. Unintended consequences, eh?
Creating EU wide standards for testing of blood, sperm and breast milk to allow greater flows across borders is a good idea. Shortages of baby formula in the US, for example, led to a valuable increase in breast milk donations and sales but it would probably be better if more breast milk donations went through a qualified milk bank rather than through Facebook (and the same is also true for sperm banks and sperm donations). But there is no call for banning paid donation.
Paying donors of blood, sperm and breast milk is an ethical way to increase the quantity supplied and it can be done while ensuring that the donations are high-quality and safe.
Compensating Kidney Donors
LA Times: Never in the field of public legislation has so much been lost by so many to one law, as Churchill might’ve put it. The National Organ Transplant Act of 1984 created the framework for the organ transplant system in the United States, and nearly 40 years later, the law is responsible for millions of needless deaths and trillions of wasted dollars. The Transplant Act requires modification, immediately.
We’ve got skin in this game. We both donated our kidneys to strangers. Ned donated to someone who turned out to be a young mother of two children in 2015, which started a chain that helped an additional two recipients. And Matt donated at Walter Reed in 2021, after which his kidney went to a Seattleite, kicking off a chain that helped seven more recipients, the last of whom was back at Walter Reed.
…The National Organ Transplant Act prohibits compensating kidney donors, which is strange in that in American society, it’s common to pay for plasma, bone marrow, hair, sperm, eggs and even surrogate pregnancies. We already pay to create and sustain life.
…Compensation models have been proposed in the past. A National Institutes of Health study listed some of the possibilities, including direct payment, indirect payment, “in kind” payment (free health insurance, for example) or expanded reimbursements. After much review, we come down strongly in support of indirect payment, specifically, a $100,000 refundable federal tax credit. The tax credit would be uniformly applied over a period of 10 years, in the amount of $10,000 a year for those who qualify and then become donors.
This kind of compensation is certainly not a quick-cash scheme that would incentivize an act of desperation. Nor does it commoditize human body parts. Going forward, kidney donation might become partly opportunistic rather than mostly altruistic, as it is now. But would it be exploitative? Not at all.
Long-time readers will know that I have argued for the greater use of incentives in organ donation both for live donors and cadaveric donors. Pecuniary compensation is one possibility but so are no-give, no-take laws that give those who previously signed their organ donor cards priority should they one day need an organ.
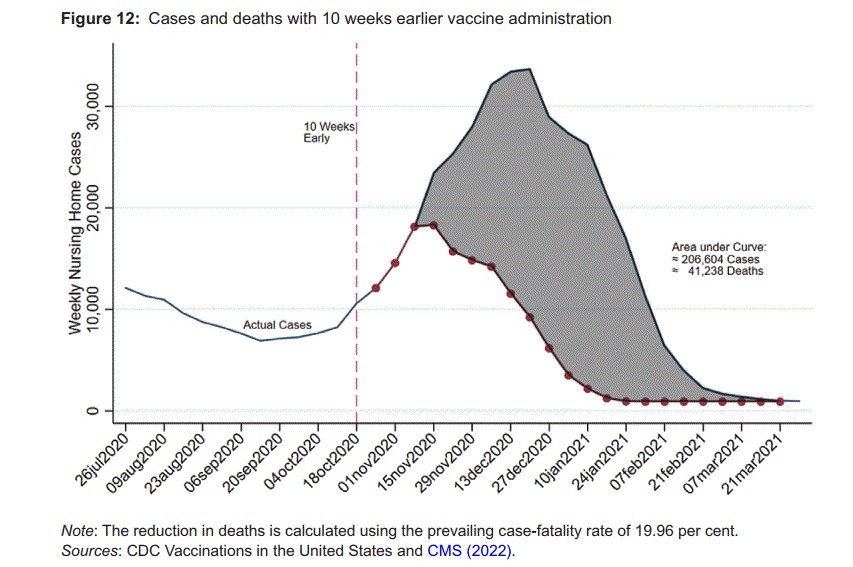
The Birx Plan for Early Vaccination of the Nursing Homes
In Covid in the nursing homes: the US experience, Markus Bjoerkheim and I show that the Great Barrington “focused protection” plan was unlikely to have worked. I covered this last week. But there was one strategy which could have saved tens of thousands of lives–early vaccination. If the vaccine trials had been completed just 5 weeks earlier, for example, we could have saved 14 thousand lives in the nursing homes alone. But put aside the possibility of completing the trials earlier. There was another realistic possibility under our noses. We had could have offered nursing home residents the vaccine on a compassionate use basis, i.e. even before all the clinical trials were completed. An early vaccination option was neither unprecedented nor a question of 20-20 hindsight, early vaccination was discussed at the time:
Deborah Birx, the coordinator of the White House Coronavirus Task Force, forcefully advocated that nursing home residents should be given the option of being vaccinated earlier under a compassionate use authorization (Borrell, 2022). Many other treatments, such as convalescent plasma, were authorized under compassionate use procedures and there was more than enough vaccine available to vaccinate all nursing home residents. As a first approximation we find the Birx plan would have prevented in the order of 200,000 nursing home cases and 40,000 nursing home deaths. To put that in perspective, it amounts to reducing overall nursing home Covid deaths by over 26 per cent (using all CMS reported resident nursing home deaths as of 5 December 2021, and estimates of underreported deaths from Shen et al. (2021)).
The lesson is not primarily about the past. It’s about the central importance of vaccines in any plan to protect the vulnerable and about how we should be bolder and braver the next time.
Addendum: See also Tyler’s tremendous post (further below) on focused protection.
Sunday assorted links
1. 41 seconds of a former CIA director on you-know-what.
2. New Substack from the great Radley Balko.
3. Should EA emulate Peak Quakerism?
4. The legal culture that is Swiss: “Lidl’s Knockoff Chocolate Bunnies Should Be Melted Down, Court Ruling Suggests.”
5. A new plan for traffic ticket enforcement.
6. Why did we wait so long for wind power?, part II.
7. False theories that explain everything: “Infected women scored higher in tribalism and lower in cultural liberalism, compared with the Toxoplasma-free control group, while infected men scored higher in economic equity.”
Tuesday assorted links
1. Motorcycles and ferries are dangerous, in that order.
2. More on civil defense in Taiwan.
3. The great Dervla Murphy has passed away.
4. Last payphone in NYC to be removed.
5. Emily Oster makes Time 100 most influential people list.
6. To what extent is tritium a limit on nuclear fusion?
7. RH being provocative (in some regards I am the opposite of his approach as outlined here).
8. Profile of Anita Summers. And in praise of Steph Curry.
9. New, skeptical study on Long Covid. And Derek Lowe with more on that.
Sunday assorted links
Friday assorted links
1. UT Austin workshop in March on Progress Studies.
2. The dating culture that is D.C., with a partial cameo by Jordan Peterson.
3. My Bloomberg column on whether we should be worried by falling crypto prices (no). And will recent SEC proposals stifle crypto?
4. Self-heating plasma and nuclear fusion.
5. Seth Curry, late bloomers?
6. In my view, David Leonhardt understands trade-offs, intertemporal substitution, the importance of economic and social life and education, and other basic concepts of thought. He is a voice of sanity. Here are a number of public health experts embarrassing themselves.
Monday assorted links
Monday assorted links
1. Jodi Ettenberg interview. Recommended.
3. Unite America, for ranked choice voting. And the sugar lobby is alive and well.
4. “We find that access to a plasma donation center reduces demand (inquiries) for payday and installment loans by 6.5% and 8.1%, respectively, with larger effects (13.1% and 15.7%, respectively) on younger borrowers. Moreover, foot traffic increases by 7-10% at essential and non-essential goods establishments when a new plasma center opens nearby. Our findings suggest that plasma donation helps households smooth consumption without appealing to high-cost debt.” Link here.
Friday assorted links
2. Vitalik on overuse of the Gini coefficient.
4. James Buchanan and club theory.
5. The details of how the delta variant works, better than I was expecting.
6. The laser-created, mid-air plasma columns hypothesis (WSJ).
7. Sriram Krishnan profile and Clubhouse (NYT).
Towards a COVAX Exchange
Israel had vaccine that was about to expire before it could be administered. South Korea needed vaccine immediately to stop a surge. They arranged a deal.
South Korea said it will receive 700,000 doses of Pfizer-BioNTech’s coronavirus vaccine from Israel on loan this week, in an attempt to speed up immunisation following a surge in infections around the capital Seoul.
…Under the vaccine swap arrangement announced by both governments on Tuesday, South Korea will give Israel back the same number of shots, already on order from Pfizer, in September and October.
South Korea has quickly distributed the COVID-19 vaccines it has, but has struggled to obtain enough doses in a timely manner as global supplies are tight, particularly in Asia.“This is a win-win deal,” [Israeli Prime Minister Naftali Bennett] said in an earlier statement.
One of the weaknesses of the COVAX facility for distributing vaccines is that distribution is primarily based on population with all countries guaranteed that “no country will receive enough doses to vaccinate more than 20% of its population until all countries in the financing group have been offered this amount.” That’s equitable, but it has dynamic challenges: different countries may have different needs and capabilities at different points in time. A country may be given vaccines, for example, when it may not yet be ready to administer them — and that can potentially lead to waste. The Israel-South Korea deal, for example, only narrowly averted 700,000 Pfizer doses from being tossed. Countries may also have different preferences for vaccines, as different vaccines may fit better with their healthcare systems. A fixed distribution schedule doesn’t adapt to the unique circumstances of time and place, as Hayek might have said.
It’s not surprising that COVAX chose a fixed distribution rule as many people wouldn’t trust a centralized authority to decide who gets what vaccines when. But what about guaranteeing each country a right to vaccine but allowing them to trade? Trade wouldn’t be vaccines for dollars which could introduce ethical and agency issues but vaccine at time 1 for vaccine at time 2 as in the Israel-South Korea exchange or across other factors such as vaccine type. My colleagues on the Kremer team, most notably Eric Budish, Scott Duke Kominers and Canice Prendergast, have been helping think through the design of just such a system. Prendergast designed the now-famous distribution system for Feeding America, Budish helped to design Wharton’s Course Match system and Kominers has worked on mechanisms for allocating convalescent plasma, vaccines and many other goods.
A suitably designed exchange can increase efficiency while maintaining equity. The Israel-South Korea deal reminds us that this is a priority. Greater efficiency in this context means fewer vaccine doses wasted, and more lives saved.