Category: Medicine
Did the Medicaid expansion limit labor force participation?
I study the effect that expanding Medicaid eligibility has on labor force participation of childless adults. The Affordable Care Act provided federal funding for states to expand public health insurance to populations that had never before been eligible for the benefit on a large scale, among those are adults without dependent children. A 2012 Supreme Court decision allowed states to choose whether or not they wanted to accept federal funds to expand Medicaid eligibility, resulting in a situation where roughly half of the population resided in states that had expanded Medicaid eligibility in 2014 and half did not. I exploit this variation by conducting a series of difference-in-differences and triple differences analyses both at a local level within one labor market, and nationwide to determine the relationship between Medicaid expansion and labor force participation. I find a significant negative relationship between Medicaid expansion and labor force participation, in which expanding Medicaid is associated with 1.5 to 3 percentage point drop in labor force participation.
That is from a Georgetown thesis by Tomas Wind, via Ben Southwood. Given the possibility of paternalistic judgments in health care policy, the simplest question here is whether this class of individuals is better off as a whole, as a result of some of them choosing this trade-off. Work is good for most people, and it is even better for their future selves, and their future children too.
Lottery Winners Don’t Get Healthier
Wealthier people are healthier and live longer. Why? One popular explanation is summarized in the documentary Unnatural Causes: Is Inequality Making us Sick?
The lives of a CEO, a lab supervisor, a janitor, and an unemployed mother illustrate how class shapes opportunities for good health. Those on the top have the most access to power, resources and opportunity – and thus the best health. Those on the bottom are faced with more stressors – unpaid bills, jobs that don’t pay enough, unsafe living conditions, exposure to environmental hazards, lack of control over work and schedule, worries over children – and the fewest resources available to help them cope.
The net effect is a health-wealth gradient, in which every descending rung of the socioeconomic ladder corresponds to worse health.
If this were true, then increasing the wealth of a poor person would increase their health. That does not appear to be the case. In important new research David Cesarini, Erik Lindqvist, Robert Ostling and Bjorn Wallace look at the health of lottery winners in Sweden (75% of winnings within the range of approximately $20,000 to $800,000) and, importantly, on their children. Most effects on adults are reliably close to zero and in no case can wealth explain a large share of the wealth-health gradient:
In adults, we find no evidence that wealth impacts mortality or health care utilization, with the possible exception of a small reduction in the consumption of mental health drugs. Our estimates allow us to rule out effects on 10-year mortality one sixth as large as the crosssectional wealth-mortality gradient.
The authors also look at the health effects on the children of lottery winners. There is more uncertainty in the health estimates on children but most estimates cluster around zero and developmental effects on things like IQ can be rejected (“In all eight subsamples, we can rule out wealth effects on GPA smaller than 0.01 standard deviations”). Overall for children:
Our results suggest that in a model of child development parameterized to match conditions in Sweden, the effect of permanent income on children’s outcomes is small. With the exception of obesity risk, we estimate precise zero or negative effects in subpopulations for which theories of child development predict larger benefits of wealth. For example, though the mechanism differs, investment models (Becker and Tomes 1979) and parental stress models (Bradley and Corwyn 2002) predict larger positive effects of wealth shocks in families with low incomes. The small impact of wealth on proxies for parenting behavior may explain why the shocks to permanent income appear to have few discernible intergenerational impacts.
One point to note is that they are looking primarily at children born prelottery although they do not find any health effects in infants born postlottery.
As the authors note, Sweden is an affluent society with an extensive social safety net. Nevertheless, there is still a significant health-wealth gradient in Sweden. We might get larger causal estimates of wealth on health elsewhere but the Swedish results bound how far we can reduce the gradient.
The bottom line: Is inequality making us sick? No.
Addendum: The methodological note below was an impressive sign of how research standards at the frontier are changing, expect to see more like this in the future:
To minimize concerns about undisclosed multiple-hypothesis testing, our intergenerational analyses were prespecified in an analysis plan posted in the public domain before running any regressions of child outcomes on the treatment variable (Cesarini et al. 2014).
Addendum 2: See the comments for useful additional information from Erik Lindqvist, one of the authors.
What is doctors’ compliance rate for hand hygiene procedures?
According to a new study, when they know they are being watched it is 57 percent.
When they don’t know they are being watched, it is 22 percent.
What I find shocking is not the difference, which fits readily into the economic way of thinking. It is that direct observation of doctors still does not get the rate above 57 percent.
Some Good News on Organ Donation
Representative Matt Cartwright (D-PA 17th District) has introduced the Organ Donor Clarification Act. The act would:
- Clarify that certain reimbursements are not valuable consideration but are reimbursements for expenses a donor incurs
- Allow government-run pilot programs to test the effect of providing non cash incentives to promote organ donation. These pilot programs would have to pass ethical board scrutiny, be approved by HHS, distribute organs through the current merit based system, and last no longer than five years.
Importantly the legislation has been endorsed by the American Medical Association and a number of other groups including Fair Allocations in Research Foundation, Transplant Recipients International Organization and WaitList Zero.
See my piece on the organ shortage in Entrepreneurial Economics and previous MR posts for more.
Why isn’t there more telemedicine?
Austin Frakt tells us:
The biggest hurdle may be state medical boards. Idaho’s medical licensing board punished a doctor for prescribing an antibiotic over the phone, fining her $10,000 and forbidding her from providing telemedicine. State laws that restrict telemedicine — for instance, requiring that patients and doctors have established in-person relationships — have drawn lawsuits charging that they illegally restrict competition. Georgia’s state medical board requires a face-to-face encounter before telemedicine can be delivered, while Ohio’s does not.
A study by Julia Adler-Milstein, an assistant professor at the School of Information and the School of Public Health, University of Michigan, found that such state laws and medical board requirements influence the extent of telemedicine use by hospitals. While 70 percent or more hospitals in Maine, South Dakota, Arkansas and Alaska use telemedicine, only 13 percent in Utah and none in Rhode Island do, for instance.
In a passionate commentary on the establishment’s hesitancy to embrace telemedicine, David Asch, a University of Pennsylvania physician, pointed out that the inconvenience of face-to-face care limits its use, but arbitrarily and invisibly. The costs of waiting and travel time and those borne by rural populations with poor access to in-person care don’t appear on the books. “The innovation that telemedicine promises is not just doing the same thing remotely,” Dr. Asch wrote, “but awakening us to the many things that we thought required face-to-face contact but actually do not.”
Here is the full NYT account.
I, medical device robotic pancreas
Third-grader Andrew Calabrese carries his backpack everywhere he goes at his San Diego-area school. His backpack isn’t just filled with books, it is carrying his robotic pancreas.
The device, long considered the Holy Grail of Type 1 diabetes technology, wasn’t constructed by a medical-device company. It hasn’t been approved by regulators.
It was put together by his father.
Jason Calabrese, a software engineer, followed instructions that had been shared online to hack an old insulin pump so it could automatically dose the hormone in response to his son’s blood-sugar levels. Mr. Calabrese got the approval of Andrew’s doctor for his son to take the home-built device to school.
The Calabreses aren’t alone. More than 50 people have soldered, tinkered and written software to make such devices for themselves or their children. The systems—known in the industry as artificial pancreases or closed loop systems—have been studied for decades, but improvements to sensor technology for real-time glucose monitoring have made them possible.
The Food and Drug Administration has made approving such devices a priority and several companies are working on them. But the yearslong process of commercial development and regulatory approval is longer than many patients want, and some are technologically savvy enough to do it on their own.
Here is the Kate Linebaugh story, interesting throughout, via Adam Thierer and Eli Dourado.
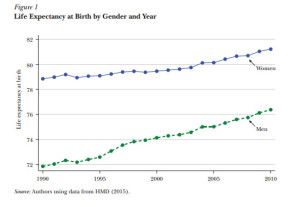
Life Expectancy is Increasing and Health Inequality is Down
We have heard a great deal about increases in mortality among white, non-hispanic, middle-aged Americans (especially women) but to state the case is also to note that this is one group among many. In an excellent new paper, Currie and Schwandt discuss the good news overall–life expectancy is up and health inequality is down, in some cases dramatically. Here, for example, is life expectancy at birth by gender and year.
 Even more impressive is that life expectancy has increased significantly across all poverty groups (as measured by county poverty levels). In the graph below, for example, the blue triangles indicate life expectancy in 1990 (men on the left, women on the right). Note that as the poverty level of the county increases along the horizontal axis life expectancy falls. The green dots are life expectancy in 2010. Once again, as poverty increases, life expectancy falls. What’s remarkable, however, is how much life expectancy increased between 1990 and 2010 in counties of all poverty levels.
Even more impressive is that life expectancy has increased significantly across all poverty groups (as measured by county poverty levels). In the graph below, for example, the blue triangles indicate life expectancy in 1990 (men on the left, women on the right). Note that as the poverty level of the county increases along the horizontal axis life expectancy falls. The green dots are life expectancy in 2010. Once again, as poverty increases, life expectancy falls. What’s remarkable, however, is how much life expectancy increased between 1990 and 2010 in counties of all poverty levels.
The news is good and may get better. Between 1990 and 2010 mortality rates for children ages 0-4 fell especially dramatically and especially so in poor counties. Moreover, since mortality at older ages is often baked in 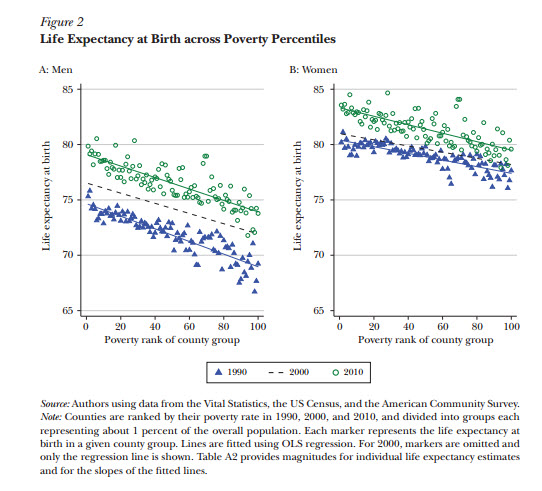 by poor health at younger ages there is significant opportunity for these gains to persist over time.
by poor health at younger ages there is significant opportunity for these gains to persist over time.
The New York Times also reported yesterday on inequality in life expectancy across race. It’s down.
Infant mortality is down by more than a fifth among blacks since the late 1990s, double the decline for whites. Births to teenage mothers, which tend to have higher infant mortality rates, have dropped by 64 percent among blacks since 1995, faster than for whites.
Blacks are still at a major health disadvantage compared with whites. But evidence of black gains has been building and has helped push up the ultimate measure — life expectancy. The gap between blacks and whites was seven years in 1990. By 2014, the most recent year on record, it had shrunk to 3.4 years, the smallest in history, with life expectancy at 75.6 years for blacks and 79 years for whites.
Part of the reason has been bad news for whites, namely the opioid crisis. The crisis, which has dominated headlines — some say unfairly, given racial disparities — has hit harder in white communities, bringing down white life expectancy and narrowing the gap.
But there also has been real progress for blacks. The rate of deaths by homicide for blacks decreased by 40 percent from 1995 to 2013, according to Andrew Fenelon, a researcher with the National Center for Health Statistics, compared with a 28 percent drop for whites. The death rate from cancer fell by 29 percent for blacks over that period, compared with 20 percent for whites.
The Currie and Schwandt paper is also very good on describing how these estimates are produced and some of the data issues with making these estimates. It’s a must read for those interested in these issues.
Demand curves slope downward, opiod edition
Deaths from opioid pain reliever overdose in the United States quadrupled between 1999 and 2013, concurrent with an increase in the use of the drugs. We used data from the Medical Expenditure Panel Survey to examine trends in opioid pain reliever expenditures, financing by various payers, and use from 1999 to 2012. We found major shifts in expenditures by payer type for these drugs, with private and public insurers paying a much larger share than patients in recent years. Consumer out-of-pocket spending on opioids per 100 morphine milligram equivalents (a standard reference measure of strength for various opioids) declined from $4.40 to $0.90 between 2001 and 2012. Since the implementation of Medicare Part D in 2006, Medicare has been the largest payer for opioid pain relievers, covering about 20–30 percent of the cost. Medicare spends considerably more on these drugs for enrollees younger than age sixty-five than it does for any other age group or than Medicaid or private insurance does for any age group. Further research is needed to evaluate whether payer strategies to address the overuse of opioids could reduce avoidable opioid-related mortality.
That is from Zhou, Florence, and Dowell, via the excellent Kevin Lewis.
The inequality that matters is doing quite well
Analysts who have concluded that inequality in life expectancy is increasing have generally focused on life expectancy at age 40 to 50. However, we show that among infants, children, and young adults, mortality has been falling more quickly in poorer areas with the result that inequality in mortality has fallen substantially over time. This is an important result given the growing literature showing that good health in childhood predicts better health in adulthood and suggests that today’s children are likely to face considerably less inequality in mortality as they age than current adults.
We also show that there have been stunning declines in mortality rates for African-Americans between 1990 and 2010, especially for black men.
Ambulances too China incentives of the day
The BBC has an interesting report on ambulance services in Beijing. Up until now, ambulance drivers could decide themselves how much to charge people for their services. I’m assuming these weren’t listed or known beforehand either. This seems ripe for abuse given that the patient will be desperately wanting to get to the hospital and in no state for bargaining. According to the article, most Chinese on social media didn’t even know that ambulances charge at all. That must come as a big shock then when they get hit up by the driver.
So what did authorities decide to do? Decree that ambulances “be fitted with taxi-style meters in an effort to allay public concerns about overcharging.” Hmm, this doesn’t seem to be the most incentive compatible policy either. As one social media cynic (read: realist) pointed out, “Don’t rule out ambulances taking a detour when using the meter.” At least when you’re in the backseat of a cab, you can watch where the driver is going. In the back of an ambulance in an emergency situation, that’s not going to be very feasible! Don’t get me wrong, I’m in no way advocating free ambulance services, but there has to be a better policy than this.
That is from Cherokee Gothic.
Another reason why Harriet Tubman is a good pick
It is also an example of great achievements in light of a disability:
As a teenager, following a severe head injury—the result of her efforts to protect another slave—Tubman developed a lifelong, chronic condition, with debilitating symptoms that have been described as being similar to those of narcolepsy and temporal lobe epilepsy.
Here is that source. Here are many other sources.
Now here’s the bad news: There is plenty in the media today about Tubman being female and black, but I haven’t seen a single story even mention this angle. Will anyone cover it? I hope so but I fear not.
Don’t count on strangers in a medical emergency
So long, good Samaritans.
In the first study of its kind, Cornell sociologists have found that people who have a medical emergency in a public place can’t necessarily rely on the kindness of strangers. Only 2.5 percent of people, or 1 in 39, got help from strangers before emergency medical personnel arrived, in research published April 14 in the American Journal of Public Health.
For African-Americans, these dismal findings only get worse. African-Americans were less than half as likely as Caucasians to get help from a bystander, regardless of the type of symptoms or illness they were suffering – only 1.8 percent, or fewer than 1 in 55 African-Americans, received assistance. For Caucasians, the corresponding number was 4.2 percent, or 1 in 24.
People in lower-income and densely populated counties were also less likely to get help, the researchers said. Conversely, those in less-densely populated counties with average socioeconomic levels were most likely to get assistance.
Here is more, via Charles Klingman.
More Lead, More Crime
In the second half of the nineteenth century, many American cities built water systems using lead or iron service pipes. Municipal water systems generated significant public health improvements, but these improvements may have been partially offset by the damaging effects of lead exposure through lead water pipes. We study the effect of cities’ use of lead pipes on homicide between 1921 and 1936. Lead water pipes exposed entire city populations to much higher doses of lead than have previously been studied in relation to crime. Our estimates suggest that cities’ use of lead service pipes considerably increased city-level homicide rates.
That’s from Feigenbaum and Muller in Lead Exposure and Violent Crime in the Early Twentieth Century. Lead, it ain’t just about Flint.
Place plays a part in helping the poor live longer
There is a new Raj Chetty paper out in JAMA ( with seven co-authors, including David Cutler), and it is garnering a lot of media attention. Here is to my mind the main result, although it is not being presented as such (NYT here):
The JAMA paper found that several measures of access to medical care had no clear relationship with longevity among the poor. But there were correlations with smoking, exercise and obesity.
I enjoyed the NYC angle from Margot Sanger-Katz:
New York is a city with some of the worst income inequality in the country. But when it comes to inequality of life spans, it’s one of the best.
Impoverished New Yorkers tend to live far longer than their counterparts in other American cities, according to detailed new research of Social Security and earnings records published Monday in The Journal of the American Medical Association. They still die sooner than their richer neighbors, but the city’s life-expectancy gap was smaller in 2014 than nearly everywhere else, and it has shrunk since 2001 even as gaps grew nationwide.
That trend may appear surprising. New York is one of the country’s most unequal and expensive cities, where the poor struggle to find affordable housing and the money and time to take care of themselves.
But the research found that New York was, in many ways, a model city for factors that seem to predict where poor people live longer. It is a wealthy, highly educated city with a high tax base. The local government spends a lot on social services for low-income residents. It has low rates of smoking and has many immigrants, who tend to be healthier than native-born Americans.
Here is the accompanying NYT graphic about “your county.” Here is Emily Badger and Christopher Ingraham, good graphics too:
The poor live shorter lives in Las Vegas, Louisville and industrial Midwest towns, such as Gary, Ind. Geography also matters much more for the poor than the rich. The health behaviors of the wealthy are similar wherever they live. For the poor, their likelihood of risky behaviors such as smoking depends a great deal on geography, on whether they live in a place where smoking is common or where, as in San Francisco, cigarettes have been shunted out of view.
It’s almost as if health care policy should be local in orientation. The link to the paper includes three comments, including one by Angus Deaton.
What happened when Easter secretly taped her surgeons
After Easter was sedated, the surgeon recounted their dispute to the other doctors. “She’s a handful,” he said in the recording. “She had some choice words for us in the clinic when we didn’t book her case in two weeks.”
“She said, ‘I’m going to call a lawyer and file a complaint,’” he recalled with a laugh. (Easter said she never mentioned a lawyer.)
“That doesn’t seem like the thing to say to the person who’s going to do your surgery,” another male voice retorted.
The comments afterward became personal. The surgeon and the anesthesiologist repeatedly referred to her belly button in jest. “Did you see her belly button?” one doctor said, followed by peals of laughter.
At another point in the procedure, the anesthesiologist appeared to refer to Easter as “always the queen,” to which the surgeon responded, “I feel sorry for her husband.”
The surgeon also used the name “Precious” several times in a manner that Easter interpreted as racial.
…After the doctors concurred that there had been many “teaching moments” that day, the anesthesiologist asked, “Do you want me to touch her?”
“I can touch her,” the surgeon is heard saying.
“That’s a Bill Cosby suggestion,” someone interjected. “Everybody’s got things on phones these days. Everybody’s got a camera.”
Here is the full story.