Results for “pandemic model” 107 found
Biden, COVID and Mental Health in America
Using US Census Household Pulse Survey data for the period April 2020 to June 2021 we track the evolution of the mental health of nearly 2.3 million Americans during the COVID pandemic. We find anxiety, depression and worry peaked in November 2020, coinciding with the Presidential election. The taking of prescription drugs for mental health conditions peaked two weeks later in December 2020. Mental health improved subsequently such that by April 2021 it was better than it had been a year previously. The probability of having been diagnosed with COVID did not rise significantly in the first half of 2021 but COVID infection rates were higher among the young than the old. COVID diagnoses were significantly lower in States that had voted for Biden in the Presidential Election. The probability of vaccination rose with age, was considerably higher in Biden states, and rose precipitously over the period among the young and old. Anxiety was higher among people in Biden states, whether they had been diagnosed or not, and whether they were vaccinated or not. The association between anxiety and depression and having had COVID was not significant in Biden or Trump states but being vaccinated was associated with lower anxiety and depression, with the effect being larger in Biden states. Whilst being in paid work was associated with lower anxiety, worry and depression and was associated with higher vaccination rates, it also increased the probability of having had COVID.
That is a new NBER working paper from the highly regarded David G. Blanchflower and Alex Bryson. Model that!
The best mask-wearing study so far?
Mask-wearing has been a controversial measure to control the COVID-19 pandemic. While masks are known to substantially reduce disease transmission in healthcare settings (Howard et al 2021), studies in community settings report inconsistent results (Brainard et al 2020). Investigating the inconsistency within epidemiological studies, we find that a commonly used proxy, government mask mandates, does not correlate with large increases in mask-wearing in our window of analysis. We thus analyse the effect of mask-wearing on transmission instead, drawing on several datasets covering 92 regions on 6 continents, including the largest survey of individual-level wearing behaviour (n=20 million) (Kreuter et al 2020). Using a hierarchical Bayesian model, we estimate the effect of both mask-wearing and mask-mandates on transmission by linking wearing levels (or mandates) to reported cases in each region, adjusting for mobility and non-pharmaceutical interventions. We assess the robustness of our results in 123 experiments across 22 sensitivity analyses. Across these analyses, we find that an entire population wearing masks in public leads to a median reduction in the reproduction number R of 25.8%, with 95% of the medians between 22.2% and 30.9%. In our window of analysis, the median reduction in $R$ associated with the wearing level observed in each region was 20.4% [2.0%, 23.3%]. We do not find evidence that mandating mask-wearing reduces transmission. Our results suggest that mask-wearing is strongly affected by factors other than mandates. We establish the effectiveness of mass mask-wearing, and highlight that wearing data, not mandate data, are necessary to infer this effect.
That is a new paper by Gavin Leech, et.al., recommended. And here is the tweet storm version of the paper.
Monday assorted links
1. Peter Singer update (New Yorker).
2. Is the frogmouth the most photogenic bird?
3. Handing out better grades is the way to get more people through college.
4. The Suwalski gap.
5. Andrew Gelman on the age-adjusted death rate, correcting an NYT claim.
6. The UK success with clinical trials.
7. Another web site for finding open vaccine spots.
8. “Last month, the cheapest rental car on Maui was a Toyota Camry for $722 a day.“
Decades of evidence on the cyclicality of real wages
I keep on hearing that “running the economy hot” is going to be very good for workers. So shall we look at the decades of evidence?
On average, the prevailing view has been that real wages are roughly acyclical across the business cycle, though with variation across and across researchers.
Here is one take from the AER:
The cyclical behavior of real wages has evolved from mildly countercyclical during the interwar period to modestly procyclical in the postwar era.
In recent times a mild acyclicality for real wages has become a more popular view, but in the 1980s it was more likely that the RBC theorists would try to show cyclicality and the aggregate demand theorists would pooh-pooh such demonstrations and insist on much weaker and theoretically ambiguous correlations. Here is an older view, incomplete in my opinion but far from absurd:
It is shown that real wages are procyclical in response to technology and oil price shocks but are countercyclical in response to aggregate demand shocks.The evidence is consistent with models where nominal wages are stickier than nominal prices
Here is a biased but interesting post Keynesian survey of the questions, with the author more or less implying we don’t know what we are talking about. Here is one of the stronger results on pro-cyclical real wages, for the EU, but it requires you to believe there is no nominal downward wage stickiness during the Great Recession (ready to bite that bullet?).
Here is a 1995 JEL survey by very good economists (Katherine Abraham and John Haltiwanger). Part of the very first sentence is:
…the debate over the cyclicality of real wages has a very long history and is filled with conflicting hypotheses and inconclusive evidence.
Here is another 1995 survey. Notice that what is probably the best and best-known attempt to explain why the cyclicality of real wages might be changing over time is built on a general equilibrium business cycle model, which has become a horror of horrors on Twitter and also in blog space.
Overall, if you study the evidence on the cyclicality of real wages you will find it is a confusing and difficult problem, and furthermore that past results may not hold in the future or for that matter in the present. Yet one rarely sees this literature, or its implications, discussed on Twitter, or for that matter on econ blogs. Here is a simple rule: if you see a discussion of current labor markets and wages, ask if the author is coming to terms with these results or not.
And I don’t know of a single research result considering macro real wages, or other labor market factors, coming out of a pandemic with suddenly available highly effective vaccines.
#thegreatforgetting
It is once again time to take scientific agnosticism seriously. Most of what you all are saying I just don’t think is founded upon very much, maybe in some cases there is n = 1 support but typically not more.
And dare I suggest that if we do not very well understand the course of wage/price over the business cycle, there is a lot more about cyclical labor markets we also don’t understand?
My excellent Conversation with John Cochrane
Here is the audio, transcript, and video. So many good parts it is hard to excerpt, here is part of the summary:
John joined Tyler to apply that habit of mind to a number of puzzles, including why real interest rates don’t equalize across countries, what explains why high trading volumes and active management persist in finance, how the pandemic has affected his opinion of habit formation theories, his fiscal theory of price level and inflation, the danger of a US sovereign debt crisis, why he thinks Bitcoin will eventually die, his idea for health-status insurance, becoming a national gliding champion, how a Renaissance historian for a father and a book translator for a mother shaped him intellectually, what’s causing the leftward drift in economics, the need to increase competition among universities, how he became libertarian, the benefits of blogging, and more.
Here is one bit from John:
COCHRANE: You ask two questions here. One is active management, and the other is trading. I’d like to distinguish them. It’s a puzzle in the Chicago free market sense.
Let me ask your question even more pointedly. If you believe in efficient markets, and you believe in competition, and things work out right, we’ve scientifically proven since the 1960s, that high-fee active managers don’t earn any more than a proverbial monkey throwing darts in a well-managed slow index. So why do people keep paying for high-fee active management?
Chicago free market — we’re not supposed to say, “Oh, people are dumb for 40 years — 50 years now,” [laughs] but there’s a lot of it. It’s one of those things. Active management is slowly falling away. The move towards passive index investment is getting stronger and stronger.
There’s a strong new literature, which I’ll point to. My colleague here, Jonathan Berk, has written some good articles on it. This is the puzzle of efficient markets. If everybody indexed, markets couldn’t be efficient because no one’s out there getting the information that makes markets efficient. Markets have to be a little inefficient, and somebody has to do the trading.
Your second question is about trading. Why is there this immense volume of trading? When was the last time you bought or sold a stock? You don’t do it every 20 milliseconds, do you? [laughs]
I’ll highlight this. If I get my list of the 10 great unsolved puzzles that I hope our grandchildren will have figured out, why does getting the information into asset prices require that the stock be turned over a hundred times? That’s clearly what’s going on. There’s this vast amount of trading, which is based on information or opinion and so forth. I hate to discount it at all just as human folly, but that’s clearly what’s going on, but we don’t have a good model.
Canada: An Official Strong Recommendation for First Doses First
Canada’s National Advisory Committee on Immunization (NACI), a scientific advisory group to the government, has made a forceful and dramatic statement strongly favoring First Doses First (delay the second dose.) This is a very big deal for the entire world. Basically NACI have endorsed everything that Tyler and I have said on First Doses First since my first post tentatively raised the issue on December 8. I am going to quote this statement extensively since it’s an excellent summary. No indentation.
—-NACI Statement—-
Based on emerging evidence of the protection provided by the first dose of a two dose series for COVID-19 vaccines currently authorized in Canada, NACI recommends that in the context of limited COVID-19 vaccine supply jurisdictions should maximize the number of individuals benefiting from the first dose of vaccine by extending the second dose of COVID-19 vaccine up to four months after the first. NACI will continue to monitor the evidence on effectiveness of an extended dose interval and will adjust recommendations as needed. (Strong NACI Recommendation)
-
- In addition to emerging population-based data, this recommendation is based on expert opinion and the public health principles of equity, ethics, accessibility, feasibility, immunological vaccine principles, and the perspective that, within a global pandemic setting, reducing the risk of severe disease outcomes at the population-level will have the greatest impact. Current evidence suggests high vaccine effectiveness against symptomatic disease and hospitalization for several weeks after the first dose, including among older populations.
Protecting individuals
- By implementing an extended four month interval strategy, Canada will be able to provide access to first doses of highly efficacious vaccines to more individuals earlier which is expected to increase health equity faster. Canada has secured enough vaccines to ensure that a second dose will be available to every adult.
- As a general vaccination principle, interruption of a vaccine series resulting in an extended interval between doses does not require restarting the vaccine series. Principles of immunology, vaccine science, and historical examples demonstrate that delays between doses do not result in a reduction in final antibody concentrations nor a reduction in durability of memory response for most multi-dose products.
- Assessment of available data on efficacy and effectiveness of a single dose of mRNA vaccine was a critical factor in assessing the impact of a delayed second dose at this time. The two available clinical trials for mRNA vaccines (Pfizer-BioNTech and Moderna) provide evidence that indicates that efficacy against symptomatic disease begins as early as 12 to 14 days after the first dose of the mRNA vaccine. Excluding the first 14 days before vaccines are expected to offer protection, both vaccines showed an efficacy of 92% up until the second dose (most second doses were administered at 19-42 days in the trials). Recently, real world vaccine effectiveness data presented to or reviewed by NACI assessing PCR-positive COVID-19 disease and/or infection from Quebec, British Columbia, Israel, the United Kingdom and the United States support good effectiveness (generally 70-80%, depending on the methodology used and outcomes assessed) from a single dose of mRNA vaccines (for up to two months in some studies). While studies have not yet collected four months of data on effectiveness of the first dose, the first two months of population-based effectiveness data are showing sustained and high levels of protection. These data include studies in health care workers, long term care residents, elderly populations and the general public. While this is somewhat lower than the efficacy demonstrated after one dose in clinical trials, it is important to note that vaccine effectiveness in a general population setting is typically lower than efficacy from the controlled setting of a clinical trial, and this is expected to be the case after series completion as well.
- Published data from the AstraZeneca clinical trial indicated that delaying the second dose to ≥ 12 weeks resulted in a better efficacy against symptomatic disease compared to shorter intervals between doses.
- The duration of protection from one or two doses of COVID-19 vaccines is currently unknown. Experience with other multi-dose vaccines after a single dose suggests persistent protection could last for six months or longer in adolescents and adults. Longer-term follow-up of clinical trial participants and those receiving vaccination in public programs will assist in determining the duration of protection following both one and two doses of vaccination. NACI will continue to monitor the evidence on effectiveness of an extended interval, which is currently being collected weekly in some Canadian jurisdictions, and will adjust recommendations as needed if concerns emerge about waning protection.
Protecting populations
- Although effectiveness after two-doses will be somewhat higher than with one dose, many more people will benefit from immunization when extending the interval between doses in times of vaccine shortage; offering more individuals direct benefit and also the possibility of indirect benefit from increasing population immunity to COVID-19 disease. Everyone is expected to obtain the full benefit of two doses when the second dose is offered after 4 months.
- Internal PHAC modelling reviewed by NACI based on Canadian supply projections suggested that accelerating vaccine coverage by extending dose intervals of mRNA vaccines could have short-term public health benefits in preventing symptomatic disease, hospitalizations, and deaths while vaccine supply is constrained. Even a theoretical scenario analysis in which intervals were extended up to six months and protection was lost at a rate of 4% per week after the first dose also showed that extending the mRNA vaccine dose intervals would still have public health benefits. External modelling results have also suggested that extending dose intervals can avert infections, hospitalizations and deaths.
- The impact on variants of concern by extending the interval between doses is unknown, but there is currently no evidence that an extended interval between doses will either increase or decrease the emergence of variants of concern. COVID-19 mRNA vaccines and AstraZeneca vaccine have shown promising early results against variant B.1.1.7. As effectiveness of the first dose against other variants of concern is emerging, ongoing monitoring will be required.
- Vaccine distribution will be optimized through this strategy, and current vaccine supply projections will work well with an extended dose strategy that aims to immunize as many Canadians as efficiently as possible. Extending the dose intervals for mRNA vaccines up to four months has the potential to result in rapid immunization and protection of a large proportion of the Canadian population….
Tuesday assorted links
1. Thwarted markets in everything: “Indianapolis Colts WR Michael Pittman Jr. says he won’t give up No. 11 to Carson Wentz.”
2. Siddhartha Mukherjee on heterogeneities in relative pandemic performance, revisiting a now-neglected topic (New Yorker).
3. North Dakota legislative house passes an anti-mask mandate bill.
4. Experiencing the Spanish flu lowered social trust. And more than 200 monoliths now.
5. Is Robert Gordon emerging from his previous stagnationist position?
6. Will/should the U.S. create a “strategic monkey reserve”? (NYT)
7. Spotify is going hi fi in selected markets. Civilization has returned (I hope).
From the Comments, On FDF
Also this from Tom Meadowcroft:
Scientific researchers search for the truth. Medical clinicians use limited data balance cost and benefits in the face of uncertainty to save the most lives.
When searching for the truth, it is important to have high standards of statistical significance, integrity, and patience, because credibility and a reputation for integrity is everything. Every academic knows that a retracted paper or an accusation of playing fast and loose with statistics can be the death knell for a career. As a result it is prudent to be very certain before publishing. Public health officials, particularly those in charge of approving vaccines, dread the possibility that a vaccine that will be given to millions of healthy people, often children, to prevent diseases where death is rare, which could harbor some flaw that causes a hundred avoidable deaths; they seek the highest standards of proof of safety and efficacy before approving such a vaccine.
But a pandemic is not a search for truth, and a COVID vaccine administered in the midst of a pandemic is very different than a measles vaccine administered to 2-year-olds. The pandemic makes these decisions for FDF or for vaccine approvals into clinical decisions, where health professionals should be balancing the certain benefit of reducing the thousands of daily deaths against the uncertain cost of the possibilities of harmful side-effects and uncertain details of efficacy (when does immunity kick in, how long does it last, how valuable is a booster) that additional months of testing and trials would reveal more clearly.
Public health researchers, academics for the most part, lack the ability (and courage) to make the sort of cost/benefit analysis with necessarily limited data that clinical physicians make every day in examination rooms. Any good clinician, faced with the citizenry of a country as their patient, would have opted for FDF, the AZ vaccine, and quite likely reduced doses by the start of the year. Because we are stuck with academics and administrators as our decision makes, unable to see beyond their usual routine of searching for the truth and protecting their reputations, thousands more will die.
Profile of Youyang Gu, data scientist
In mid-April, while he was living with his parents in Santa Clara, Calif., Gu spent a week building his own Covid death predictor and a website to display the morbid information. Before long, his model started producing more accurate results than those cooked up by institutions with hundreds of millions of dollars in funding and decades of experience.
“His model was the only one that seemed sane,” says Jeremy Howard, a renowned data expert and research scientist at the University of San Francisco. “The other models were shown to be nonsense time and again, and yet there was no introspection from the people publishing the forecasts or the journalists reporting on them. Peoples’ lives were depending on these things, and Youyang was the one person actually looking at the data and doing it properly.”
The forecasting model that Gu built was, in some ways, simple. He had first considered examining the relationship among Covid tests, hospitalizations, and other factors but found that such data was being reported inconsistently by states and the federal government. The most reliable figures appeared to be the daily death counts. “Other models used more data sources, but I decided to rely on past deaths to predict future deaths,” Gu says. “Having that as the only input helped filter the signal from the noise.”
The novel, sophisticated twist of Gu’s model came from his use of machine learning algorithms to hone his figures.
Here is the full Bloomberg piece by Ashlee Vance, I am especially pleased because Youyang was an Emergent Ventures winner. Here is Youyang Gu on Twitter.
The economic geography of global warming
By Jose Cruz Alvarez and Esteban Rossi-Hansberg:
Our baseline results show welfare losses as large as 15% in parts of Africa and Latin America but also high heterogeneity across locations, with northern regions in Siberia, Canada, and Alaska experiencing gains. Our results indicate large uncertainty about average welfare effects and point to migration and, to a lesser extent, innovation as important adaptation mechanisms.
A few points:
1. Average global welfare loss is about six percent. The discount rate is 0.9%, and yes those are welfare losses. Losses as a percent of gdp are somewhat lower, because amenity costs are a factor with global warming.
2. About half of the global losses stem from the negative effects on productivity. For Africa, amenities losses are especially important. Overall the biggest losers are Central America, India, Brazil, and Africa. Many colder regions are better off.
3. The model allows for many margins of adjustment, including migration. Cheaper/freer migration is a good way of limiting the costs from global warming.
4. Subsidies to green energy don’t help very much, because of Jevons-like effects, namely that energy becomes cheaper and total energy use rises.
5. A carbon tax postpones fossil fuel use but in the long run it doesn’t help much, unless the delay in fossil fuel extraction is used to buy effective abatement measures.
Of course the assumptions in such papers always can be challenged, but this is one case where the authors think like economists throughout the entire exercise. It seems to be one of the best such studies.
My net conclusion (not theirs) is that the paper shows why serious action has been so slow in coming. The world as a whole might lose about two years worth of economic growth, with most of the losses concentrated in countries that are not calling the shots. Let’s say a poor country loses fifteen percent of welfare and about ten percent of gdp. Isn’t that somewhat similar to many of the losses caused by the current pandemic? Circa early 2021, how many vaccines are we sending to those places?
I do fully agree that we should be more cosmopolitan, but first to fix the malady we must understand it.
The Big Push: A Plan to Accelerate V-Day
In the Washington Post I have an extensive piece on accelerating progress to V-day, Vaccine or Victory day, the day everyone who wants a vaccine has gotten one. I cover themes that will be familiar to MR readers, including First Doses First, Fractional Dosing, Approving More Vaccines and DePrioritization to Expand Delivery. I won’t belabor these points here but the piece is useful at collecting all the arguments in one place and there are lots of authoritative links.
One point I do want to make is that all the pieces of the “Tabarrok plan,” if you will, fit together. Namely, use First Doses First to make a big push to get as many people vaccinated with first doses as possible in the next 90 days. Approve more vaccines including Johnson & Johnson, AstraZeneca and others and make them available to anyone, anywhere–that is possible because these vaccines don’t require significant cold storage, J&J is a single shot and AZ is better with a second shot at 12 weeks or later all of which eases distribution.
…some people argue that adding a third (or fourth) vaccine might not help because of persistent delivery logjams at the state and local levels. But we know there is unused distributional capacity, even for the supply we do have. The United States is currently administering about 1.5 million coronavirus vaccine shots per day. While that sounds like a lot, for comparison consider that in September — during the pandemic, when social distancing measures were in full effect — we vaccinated for the seasonal flu in some weeks at the rate of 3 million people a day.
There are two main reasons the rollout has been so slow. First, the Moderna and especially the Pfizer vaccines require ultracold storage. (The Johnson & Johnson and AstraZeneca doses can be stored at ordinary refrigerator temperatures.) Second, we have tried to prioritize vaccinations using a confusing mishmash of age, health conditions and essential-worker status that differs by state and sometimes even by county. “Confirming such criteria is complicated at best, and it’s probably not even feasible to try under conditions of duress,” as Baylor’s Hotez puts it.
Arguments continue about prioritization lists, and the idea of tossing them entirely would cause a political fight. But there is a compromise at hand: Quickly approve the Johnson & Johnson and AstraZeneca vaccines and make them — and only them — available to anyone, anywhere. Keeping things simple is a sure way to increase total vaccinations. With no cold-storage requirement, the new vaccines could be administered by any of the 300,000 pharmacists and more than 1 million physicians in the United States authorized to deliver vaccines, most of whom are not now giving Pfizer or Moderna shots.
Tuesday assorted links
1. Is the English strain picking up some features of the South African strain? And the new strains do seem somewhat more dangerous.
2. Joe Stiglitz comes perilously close to the Austrian theory of the business cycle.
3. Update on the Russian vaccine (New Yorker). And this WSJ piece. It seems to work? And yet more.
4. ““What we didn’t anticipate was that they would break the law,” Goldenfeld said — that some students, even after testing positive and being told to quarantine, would attend parties anyway.” A look at some of the models.
5. “Dubai announced Monday the creation of a “space court” to settle commercial disputes, as the UAE — which is sending a probe to Mars — builds its presence in the space sector.” Link here.
6. My on-line talk to PayPal. Mostly Q&A, and they did ask me about Nirvana’s “Aneurysm.”
Saturday assorted links
1. Rap song about Janet Yellen.
2. Never too much talent? Should you be bullish on the Nets?
3. Toward a more libertarian pandemic?
5. B.1.1.7 not in decline. And that variant is exploding in Denmark.
6. Vaccines to take Israel back from the Ibex, photo gallery, recommended. And some verticality in a video version. Consider it “the Ibex salt-water paradox.”
7. Peter Huber tribute, he has passed away.
Friday assorted links
2. Don Boudreaux open letter to me. Here is my original post, and here is AIER being useful. If the GBD had been this second link here, I would be wrong. But it wasn’t.
3. Chinese to vaccinate 50 million for lunar new year.
4. Model and evidence for the IPO market being efficient.
5. Why Iger is a bad pick for ambassador to China.
6. Whether you agree or not, the method and approach of the government/CDC here on vaccine allocation are so low quality as to almost defy belief. Again, whether or not you are convinced by Matt Yglesias, his simple Substack on this same question did a better job (and at a profit, presumably!). A useful reminder for those of you who “blame the CDC problems on Trump.” Here is related NYT coverage. And never forget Glazer. Why do we not prioritize men, who are at higher risk? And from “an expert in ethics.”
8. “Atlantic City has launched an auction in which the winner will get to virtually push the button that starts the long-anticipated implosion of the former Trump Plaza Hotel and Casino building.” Link here.
The Simple Math of FDA Delay
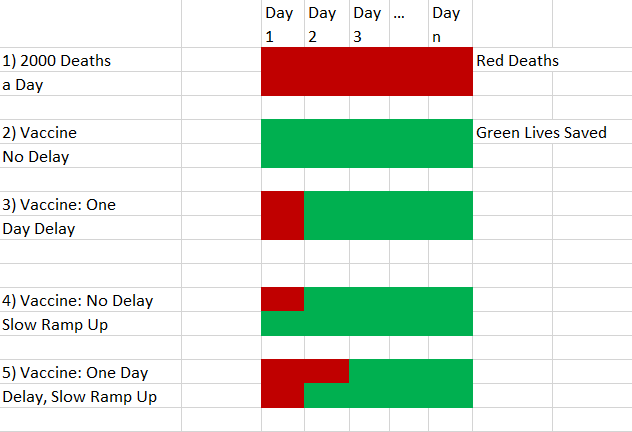
Two to three thousand people a day are dying from COVID. Thus anything that delays rolling out a vaccine has a very high cost in human lives. People want to deny this, perhaps because it is so horrifying. I get a lot of pushback when I say that FDA delay is deadly. Let’s dispense with a few objections. It is true, of course, that the people who are dying today can’t literally be saved by a vaccine today but they could have been saved had they been vaccinated four or five weeks ago and similarly projecting forward.
Another response that many smart people tell me is that a vaccine can’t be rolled out immediately so even under the best scenarios you couldn’t save that many people immediately. That’s true but irrelevant. Since a lot of people are getting this wrong, I want to show this in a simple model using pictures. Red is for deaths. Green is for life. Suppose two thousand people are dying from COVID a day as in panel 1. Let’s for the sake of the simple model assume that you could deliver a vaccine to everyone on Day 1. You would then save 2000 lives a day going forward for however long the pandemic would have lasted as shown in panel 2. If you delay by one day then two thousand people die who would have lived without the delay, as shown in panel 3. Pretty obvious so far.
Now assume that the vaccine can’t roll out to everyone immediately. For the sake of this simple model let’s assume that on day one you can only vaccinate half the population. By doing so you save 1000 lives on day 1 and 2000 lives every day thereafter for the length of the pandemic. That’s the fourth panel. Now suppose we delay the vaccine rollout by one day. 2000 people die on Day 1 but you save 1000 on Day 2 and 2000 on Day 3 and every day thereafter for the length of the pandemic. How many people were killed by the delay? Compare the 4th and 5th panels. 2000 exactly as before! The slow ramp up doesn’t change the number of deaths caused by delay it just spreads them out over different days. You can adjust the ramp so that it occurs over 10 days or 30 days. Doesn’t change much on the delay margin unless you delay for so long that the pandemic is close to being over.
What could matter is if delay increases the speed at which you can ramp up. I doubt that this is true. We were ready to go with millions of doses in late October (guess why?). (In fact we had a vaccine in January and millions of doses around March-April.) We won’t really be better prepared tomorrow than we are today. It’s learning by doing that matters. See the point Tyler made earlier about economic time versus calendar time.
As Tyler noted, this is hardly the final analysis but many people are not even conceptualizing the problem correctly and this is a good place to begin.
Sure and Tom Meadowcroft have been hitting it out of the ballpark in the comments sections. Two examples.
Sure: