Results for “first doses first” 105 found
Medical ethics? (model this)
Steven Joffe, MD, MPH, a medical ethicist at the University of Pennsylvania, said he doesn’t believe clinicians “should be lowering our standards of evidence because we’re in a pandemic.”
Link here. That sentence is a good litmus test for whether you think clearly about trade-offs, statistical and speed trade-offs included, procedures vs. final ends of value (e.g., human lives), and how obsessed you are with mood affiliation (can you see through his question-begging invocation of “lowering our standards”?). It is stunning to me that a top researcher at an Ivy League school literally cannot think properly about his subject area at all, and furthermore has no compunction admitting this publicly. As Alex wrote just earlier today: “Waiting for more data isn’t “science,” it’s sometimes an excuse for an unscientific status-quo bias.”
To be clear, we should run more and better RCT trials of Ivermectin, the topic at hand for Joffe (and in fact Fast Grants is helping to fund exactly that). But of course the “let’s go ahead and actually do this” decision should be different in a pandemic, just as the “just how much of a hurry are we in here anyway?” calculus should differ as well. I do not know enough to judge whether Ivermectin should be in hospital treatment protocols, as it is in many countries, but I do not condemn this simply on the grounds of it representing a “lower standard.” It might instead reflect a “higher standard” of concern for human lives, and you will note the drug is not considered harmful as it is being administered.
If you apply the standards of Joffe’s earlier work, we should not be proceeding with these RCTs, including presumably vaccine RCTs, until we have assured that all of the participants truly understand the difference between “research” and “treatment” as part of the informed consent protocols. No “therapeutic misconception” should be allowed. Really?
If the pandemic has changed my mind about anything, it is the nature of expertise.
Canada and Novavax
Canada has made some smart moves with the Novavax vaccine. First, they initiated a rolling review of the Novavax vaccine in late January which suggests that they might authorize the vaccine based on the British trial before the US trial is concluded. The FDA will probably wait until the US trial is concluded. Second, Canada also signed a production agreement to bring some capacity online in Canada, although that will take time. That agreement, however, is on top of an advance purchase of 52 million doses with an option on another 24 million doses.
In short, if they act quickly, Canada could approve the Novavax vaccine before the United States and get a jump on its own vaccination efforts.
Vaccine politics in Europe and America
The contentiousness is much worse in Europe, where zero- and negative-sum thinking is the order of the day. That is the theme of my latest Bloomberg column, here is one bit:
In most of Europe, it’s hard to see much good news. It’s one thing not to have a vaccine. It’s far worse to turn on television or go on the internet and see people in other countries being vaccinated as their pandemics recede. Most of Europe will not be making significant vaccination progress until April, and even then shortages may remain.
At stake is the very legitimacy of the EU. Most of the vaccination contracts were handled at the EU level, although Germany sidestepped the agreed-upon procedures and cut some deals. If the EU fails at the most significant crisis in a generation, it may not maintain much legitimacy.
And:
When people judge how painful an experience was, they often place a high value on first and last impressions. The last impressions of the U.S. and U.K. will be pretty positive. Most of the U.S. pandemic will be over by July, even under a subpar vaccination schedule. And it may turn out that mRNA vaccines are more protective against the new strains of Covid than any alternatives….
Many European countries may end up with fewer deaths per capita than the U.S. But at the end of the pandemic many Europeans may feel like their leaders failed them, that they suffered lockdowns for many months but received little in return. Right now vaccine politics is all about momentum, and so far only a few countries have it.
Here is a related piece by Bruno M. And a good piece (slow to start) on what went wrong in the EU.
To Every One Who Has, More Will Be Given
From an email to Fairfax County teachers:
Due to a decrease in vaccine allocation, we are temporarily reducing appointment availability over the coming weeks. Vaccine supply is fluid across the country, and we are matching currently scheduled appointments to anticipated inventory.
We are pleased to share that more than 22,000 Fairfax County Public Schools teachers and employees have already been able to schedule their first shot. At this time we are honoring those who have current appointments. Should our vaccine supply not be sufficiently replenished, we will suspend initial appointments (first doses) for eligible individuals in 1b and prioritize those who require their second vaccine dose in the weeks to come.
It’s really quite stunning when you think about it.
Hat tip: Max.
Vaccines Are Not Like Emergency Rations!
According to the Guardian the First Minister of Wales explained their policy of doling out the Pfizer vaccine evenly over the next six weeks:
the Pfizer vaccine has to last us until into the first week of February.
…We won’t get another delivery of the Pfizer vaccine until the very end of January or maybe the beginning of February, so that 250,000 doses has got to last us six weeks.
That’s why you haven’t seen it all used in week one, because we’ve got to space it out over the weeks that it’s got to cover.
Bonkers! A vaccine isn’t like a limited supply of water that needs to be rationed until you arrive at the next oasis. The sooner you get the vaccine out the better! Start lowering R now! If you run out of vaccine, well scarcity is bad but running out means that at least one part of your system is working well! It’s a bad idea to kill people to make it look like you are following some sort of numerically neat plan.
One year into the pandemic and people still don’t understand vaccines or viral growth.
Hat tip: Arthur Baker.
Fact of the day, get to those rooftops!
Pepvar’s first goal should be supporting the production of enough doses to vaccinate the entire world within a year. It is estimated that building such capacity for an mRNA vaccine like Moderna’s would cost less than $4 billion — that’s significantly less than the U.S. government already spends each day on Covid-19 relief — with the cost about $2 per dose. Of course, making the vaccines is just the first step: Pepvar must
People, even if that estimate is off by a factor of ten or more…etc. Here is the NYT link, bJames Krellenstein, Peter Staley and .
The Tony Blair “one dose” idea
Here is the source, of course Alex Tabarrok was there first. For now give everyone one dose rather than two, and enjoy the partial but more broadly spread protection. Here are the reactions from two epidemiologists:
Professor Wendy Barclay, from the department of infectious disease at Imperial College London, said Mr Blair’s idea was interesting but agreed it was “too risky” to try without further evidence.
And Professor Neil Ferguson, also from Imperial, added that the UK regulator had authorised the vaccine on the basis that people would receive two doses.
Administering one dose only would require “an entirely different regulatory submission”, he told a Commons committee.
A Department of Health and Social Care spokesperson said: “Over the coming weeks and months, the rate of vaccinations will increase as more doses become available and the programme continues to expand.”
Where are their cost-benefit analyses? Letting people get infected at current and indeed accelerating rates is also “too risky,” yes? Is there an epidemiologist or public health expert out there willing to show his or her work, either for or against this idea? A genuine query, and of course comments are open. How about one dose for Moderna only? If we are to defer to their expertise, they do actually have to step up and be the experts, right?
Double the Inoculated Population with One Dose
I’ve been arguing that we should delay the second dose (or at least not hold back first doses) in order to hit the virus hard and inoculate more people on the first dose. I wrote:
We should vaccinate 6 million people with first dose NOW. It is deadly cautious to hold second dose in *reserve*. Supply chain will be ok and the exact timing of the second dose is not magical and likely not critical. In the accidental low-dose, standard-dose regime for the AZ vaccine, people got the second dose 7 to 8 weeks after the first dose and that was the 90% efficacious regime. [A different vaccine obviously but ] Exact timing of the second-dose does not seem critical, although everyone should get a second dose.
Today epidemiologist Michael Mina and writer Zeynep Tufekci, who has been ahead of the curve on much of the discussion, make the case even more strongly in the NYTimes:
First, the science. While the vaccine trials were designed to evaluate a two-dose regimen, some immunity might be acquired before a second dose is administered. We know, for instance, that a Covid-19 infection appears to yield protection for at least six months. While infections are not vaccinations, and while we need more data on this, it’s plausible that the immunity gained from a vaccination may turn out to be even stronger than what comes from an infection. The reason we do a second — booster — vaccination is that these later doses help to solidify immune memory, in part by giving extra training to the cells that produce antibodies, a process called affinity maturation. But this process begins with the single dose, and the evidence collected between the time of the first and second doses in tens of thousands of people in the Phase 3 trials suggests that the level of affinity maturation may provide enough protection to meet the standards we have set for vaccine approval during this pandemic even without the second dose.
While we know that the single dose can protect against disease, we don’t yet know how long this immune protection will last, and at what level. However, there is no rule that says that vaccines must be boosted within weeks of each other. For measles, the booster dose is given years after the first dose. If the booster dose could be given six months or a year after the first dose, while maintaining high efficacy before the second dose, that would allow twice as many people to get vaccinated between now and later next year, accelerating herd immunity — greatly helping end the crisis phase of the pandemic in the United States.
… we should begin immediate single-dose trials, recruiting volunteers from low-risk populations who are first in line for the vaccinations. For example, among health care workers protective equipment works, rates of infection among this group have fallen sharply and severe disease is much more rare.Younger essential workers without risk factors are less likely to be severely affected if they are exposed since this disease’s impact rises steeply with age. Just as tens of thousands of people volunteered for the earlier vaccine trials, many may well volunteer to test a placebo against a second dose, allowing us to quickly ascertain questions of durability and effectiveness of the single dose.
Two additional points. First, mix and match, as I argued earlier, may be beneficial:
…we could mix and match vaccines. The UK will run a trial on this question. Mix and matching has two potentially good properties. First, mix and matching could make the immune system response stronger than either vaccine alone because different vaccines stimulate the immune system in different ways. Second, it could help with distribution. It’s going to be easier to scale up the AZ vaccine than the mRNA vaccines, so if we can use both widely we can get more bang for our shot.
Second, an economics issue. If we want Pfizer and Moderna on board we need to pay them not just to run the clinical trials but to be happy with potentially selling half as many doses. Incentives matter.
The Vaccine Works Fast
From the FDA report:
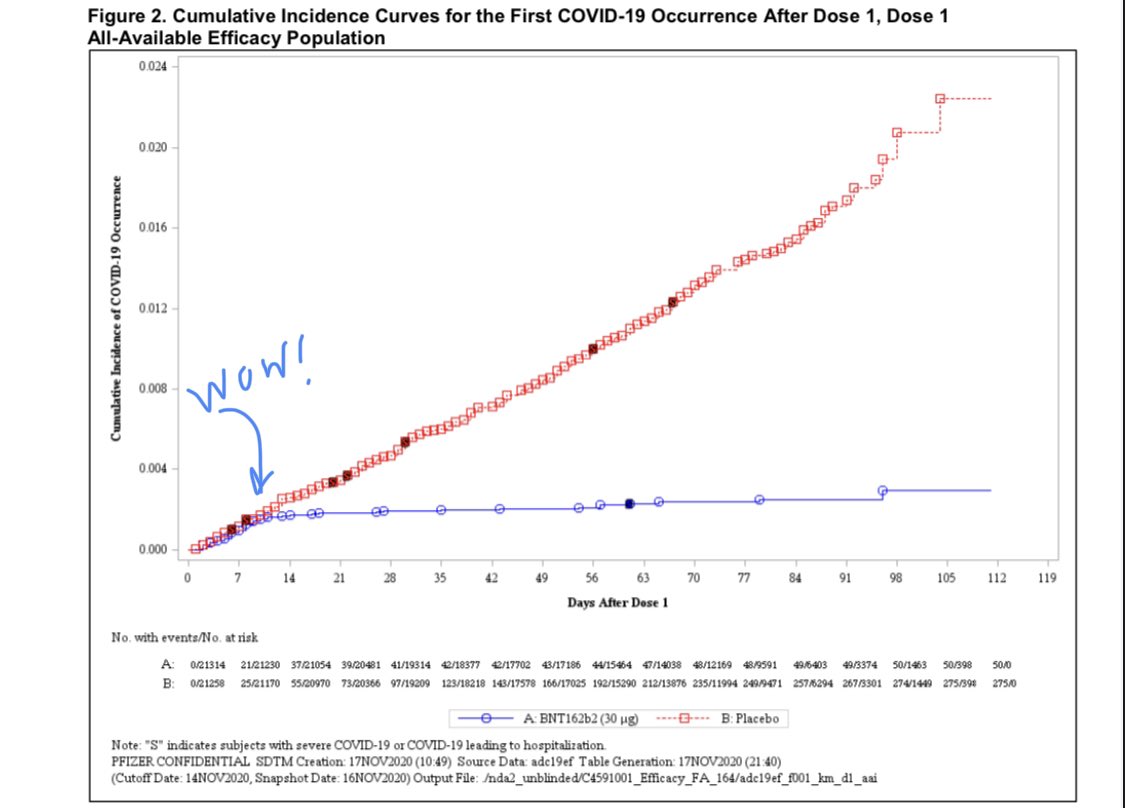
Two doses is great but one dose already looks good even though sample is small. “Efficacy against severe COVID-19 occurring after the first dose was 88.9%.” (Added. n.b this is over the entire sample.)
Based on the number of cases accumulated after Dose 1 and before Dose 2, there does seem to be some protection against COVID-19 disease following one
dose; however, these data do not provide information about longer term protection beyond 21 days after a single dose.
This is potentially important as we could vaccinate more people in a hot-spot and potentially delay the second dose. Noting, however, that this is a post-hoc analyses and the second dose came within 3 weeks.
As expected, a bit of pain, swelling and fatigue in a minority of participants are the biggest issues. No major safety concerns. Of course, we still need to monitor long-term.
Serious adverse events, while uncommon (<1.0%), represented medical events that occur in the general population at similar frequency as observed in the study…. No specific safety concerns were identified in subgroup analyses by age, race, ethnicity, medical comorbidities, or prior SARS-CoV-2 infection.
Hat tip: Biostatistician LucyStats.
The case for going big is still strong
Since back in April, Michael Kremer, myself, and the AHT team have been advising governments to go big on investing in vaccines. The US, to its credit, made early purchases but they made two mistakes. First, they didn’t buy enough as the Washington Post indicates:
Last summer, Pfizer officials had urged Operation Warp Speed to purchase 200 million doses, or enough of the two-shot regimen for 100 million people, according to people knowledgeable about the issue who spoke on the condition of anonymity because they weren’t authorized to discuss the situation. But the Warp Speed officials declined, opting instead for 100 million doses, they said.
“Anyone who wanted to sell us … without an [FDA] approval, hundreds of millions of doses back in July and August, was just not going to get the government’s money,” said a senior administration official.
But last weekend, with an FDA clearance expected any day, federal officials reached back out to the company asking to buy another 100 million doses. By then, Pfizer said it had committed the supply elsewhere and suggested elevating the conversation to “a high level discussion,” said a person familiar with the talks who spoke on the condition of anonymity because they were not authorized to share the conversation.
In our discussions, we were talking about at least a $70 billion dollar program and optimally double that and we continually faced the sticker shock problem. Investing in unapproved vaccines seemed risky to many people despite the fact that the government was spending trillions on relief and our model showed that spending on vaccines easily paid for itself (the mother of multipliers!). I argued that this was the world’s easiest cost benefit calculation since Trillions>>Billions. But it was hard to motivate more spending—not just in the United States but anywhere in the world. For reasons I still don’t understand anything out of the ordinary–big spending on at-risk vaccines, spending on testing and tracing, challenge trials–was met with a kind of apathy and defeatism. As I said in July:
Multiple people [in Congress] have told me that things move slowly, no one is stepping up to the plate, leadership is absent. “Who is John Galt?,” they sigh. Ok, they don’t literally say that, but that sigh of resignation is what it feels like in the United States today at the highest levels of government.
OWS was actually the one area where there was some action. But there was a second mistake. We argued that governments shouldn’t buy doses but capacity, i.e. they should cover the cost of building a factory or production line in return for an option on doses from that line. The problem with buying doses is that if you buy without a timeline then the company takes all orders and pushes the low-priced orders to the back of the queue. If you demand a timeline, however, that puts a lot of risk on the firms, since not everything is under their control, and that’s expensive and difficult to contract for and monitor. Thus, we advocated for push funding to de-risk capacity construction for the firms. Capacity construction is well understood–double this line–and thus much easier to contract for and monitor. (Contracting on capacity is also cheaper than a traditional AMC for reasons explained here and also in my discussion with Tyler here.) The nice thing about buying capacity is that it changes the dynamic from one where countries are scrambling to buy before others do to one where early purchases increase capacity that is later available for everyone. OWS, to its credit, did fund capacity construction for Moderna but we wanted more and other governments didn’t step up to the plate.
OWS has been a success. In combination with investments from other governments and organizations like CEPI it will save trillions of dollars and many lives. It could have been better but the main takeaway is that the case for going big is still strong. We have solved the scientific problem of making the vaccine but step two is getting billions of doses in arms. If we can increase capacity enough to vaccinate millions more people next year than currently planned that would still pay for itself many times over. Increasing capacity is not impossible. China is increasing capacity for its vaccines. It will be harder to increase capacity for mRNA vaccines since the technology is new and bespoke but it can be done. We need a second Operation Warp Speed, OWS: Delivery and Distribution.
As Tyler said yesterday, Williams wants a cow! We want billions of vaccine doses quickly. It can be done, it should be done.
India vaccine markets in everything
Doses of the coronavirus vaccine developed by AstraZeneca and the University of Oxford could be available for purchase in India as soon as March, according to one manufacturer, in the first sign that the sought-after jab will make its way on to the private market.
Serum Institute of India, the world’s largest vaccine manufacturer, has a licence to produce the shot and has already manufactured 40m doses. Once the job is approved for use, Serum will initially supply the Indian government but then expects to sell 20m-30m doses to private facilities, according to Adar Poonawalla, chief executive.
“Everybody’s asking ‘When can I access the vaccine?’ I’ve told those guys it’s probably going to be March or April,” Mr Poonawalla told the Financial Times.
…the future availability of vaccines for sale privately in other countries, such as India, increases the likelihood of a secondary market developing for vaccines where locals or foreign visitors could pay for a vaccination if not eligible to be inoculated under their own government’s scheme.
Here is the full FT article, via J., the price is expected to be around eight dollars.
The political economy of Swine flu vaccine allocation
Previous research has isolated the effect of “congressional dominance” in explaining bureaucracy-related outcomes. This analysis extends the concept of congressional dominance to the allocation of H1N1, or swine flu, vaccine doses. States with Democratic United States Representatives on the relevant House oversight committee received roughly 60,000 additional doses per legislator during the initial allocation period, though this political advantage dissipated after the first 3 weeks of vaccine distribution. As a result political factors played a role in determining vaccine allocation only when the vaccine was in particularly short supply. At-risk groups identified by the Centers for Disease Control (CDC), such as younger age groups and first responders, do not receive more vaccine doses, and in fact receive slightly fewer units of vaccine.
That is from an Economic Inquiry paper by Matt E. Ryan. Via Henry Thompson.
Graduating in a Recession Can Be Rough
Graduating in a recession can be rough. Wages start lower and advance more slowly. It’s hard to get hired at a top firm which means it takes longer to get on a rapid ascent career path. As Till von Wachter notes in a review of the long-term consequences of initial labor market conditions, failure to takeoff leads to choices which often makes things worse.
…initial labor market conditions persistently increases excessive alcohol consumption (Maclean 2015) and leads to higher obesity and more smoking and drinking in middle age (Cutler, Huang, and Lleras-Muney 2015)…College graduates entering during the 1980s recession experience higher incidence of heart attacks in middle age (Maclean 2013). Following all labor market entrants from these cohorts, Schwandt and von Wachter (2020) find that starting in their late 30s, unlucky entrants begin experiencing a gap in mortality compared to luckier peers that keeps increasing in their 40s, driven by higher rates of heart disease, liver disease, lung cancer, and drug overdoses.
…Marital patterns of unlucky cohorts are affected from the time they enter the labor market up into middle age, when these cohorts have fewer children (Currie and Schwandt 2014), are more likely to have experienced a divorce, and are more likely to live on their own (Schwandt and von Wachter 2020). Initial labor market conditions also have been found to have effects on attitudes towards economic success and the role of the government (Giuliano and Spilimbergo 2014) and to lead to increasingly lowering individuals’ self esteem (Maclean and Hill 2015).
Don Peck had a good popular survey of these effects in The Atlantic in 2010 that remains vital:
Andrew Oswald, an economist at the University of Warwick, in the U.K., and a pioneer in the field of happiness studies, says no other circumstance produces a larger decline in mental health and well-being than being involuntarily out of work for six months or more. It is the worst thing that can happen, he says, equivalent to the death of a spouse, and “a kind of bereavement” in its own right. Only a small fraction of the decline can be tied directly to losing a paycheck, Oswald says; most of it appears to be the result of a tarnished identity and a loss of self-worth. Unemployment leaves psychological scars that remain even after work is found again, and, because the happiness of husbands and the happiness of wives are usually closely related, the misery spreads throughout the home.
Especially in middle-aged men, long accustomed to the routine of the office or factory, unemployment seems to produce a crippling disorientation. At a series of workshops for the unemployed that I attended around Philadelphia last fall, the participants were overwhelmingly male, and the men in particular described the erosion of their identities, the isolation of being jobless, and the indignities of downward mobility.
Of course, most people who graduate during a recession do just fine in the grand scheme of things.You could have graduated in Sierra Leone. But if you want to be on a rapid ascent career path remember that your first job is not your last job, look for opportunity, and be prepared to take a risk and switch jobs early. Stay off drugs and alcohol.
From the comments, on HCTs
The box most bioethicists are in is so small their thinking can’t extend beyond a few target people. In this case, the control group in a vaccine trial.
The subjects could be paid for the risk, which is what we do for jobs all the time. Those risk/reward amounts for risky jobs are used to make estimates for the value of human life. Life insurance would allow high-risk people (us geezers) to join the trials.
Their box doesn’t even consider human challenge trials (HCT) that give you very rapid and accurate data on efficacy even with pay and insurance to cover the risk. The lives saved by a month faster approval is in the 10’s of thousands more than offsetting and risk to a few people. Tracking the first million doses for side effects would provide the side effect data that is usually within days of injection.
Outside their mental box, 1000 people per day are dying for each day they study the issue and delay a decision, but those lives are not included in their thinking and analysis.
That is from Dallas. I would stress there are higher costs yet from delay, noting the hundreds of millions of people in developing nations who are falling back into poverty while the pandemic continues to rage. Some of them are dying too.
New results on the Chinese vaccine
Importantly, this was the first study of an inactivated SARS-CoV-2 vaccine to include participants older than 60 years—the most vulnerable age group for this infection. In the phase 1 dose-escalating trial, the vaccine was given at a two-dose schedule at three different concentrations (2 μg, 4 μg, and 8 μg per dose) and was well tolerated in both age groups (18–59 years and ≥60 years). The older age group had lower rates of solicited adverse events than the younger adults: the overall rates of adverse events within 28 days after vaccination were 34 (47%) of 72 participants in the group aged 18–59 years, compared with 14 (19%) of 72 participants in the group aged 60 years and older. At the same time, in both age groups the vaccine was similarly immunogenic: the geometric mean anti-SARS-CoV-2 neutralising antibody titres measured by a 50% virus neutralisation assay 14 days after the booster dose were 88, 211, and 229 in the group aged 18–59 years and 81, 132, and 171 in the group aged 60 years and older for 2 μg, 4 μg, and 8 μg vaccine doses, respectively. Moreover, the authors tested cross-reactivity of the neutralising antibodies against several drifted SARS-CoV-2 isolates and showed the potential of their vaccine to protect against evolutionary diverged viruses, should they appear in circulation.
And:
The current study is the second to report the interim results of safety and immunogenicity of inactivated SARS-CoV-2 vaccine, with the first being the another β-propiolactone inactivated aluminium-adjuvanted whole-virion SARS-CoV-2 vaccine developed by Wuhan Institute of Biological Products.
Both studies showed very similar levels of adverse events and neutralising antibody titres post vaccination, which indicates the reproducibility of clinical results of similar vaccine modes produced by different manufacturers.
All good news of course, and this vaccine exists right now. Just not for you! Here is the piece from The Lancet, and here is associated commentary, also seeming to confirm the positive results. A phase III trial is underway in the UAE to measure efficacy. I cannot speak to data reliability issues, but presumably the referees at The Lancet find this credible enough to recommend publication.
Via Alan Goldhammer.