Category: Medicine
Price Controls and the Medicare Bill
I agree with Tyler that the special interest subsidies in the new Medicare law are outrageous, albeit to be expected. What really depresses me, however, is not the subsidies (which are mostly transfers) but that we are now on an inevitable path towards price controls on pharmaceuticals. True, the law as written explicitly forbids this but political pressure will burst that dam of parchment. (Recall that the original Medicare act forbid the federal government from exercising control over the practice of medicine – try telling that to a doctor today.) Costs will soar as increased demand pushes up prices and more people are added to the program and when this happens the public will demand controls. With controls you can expect significant curtailment of R&D in new pharmaceuticals. I only hope that the drugs that will help me deal with my old age will already have been discovered.
The new Medicare bill
I am growing tired of attacking this bill, but here is another good link, from The Boston Globe, for my other writings on the topic scroll down through the last two weeks. The authors write:
In the name of greater free-market competition, the legislation offers massive new subsidies to the pharmaceutical and insurance industries. In the name of providing greater protection, it threatens Medicare’s guarantee of universal benefits. (Indeed, it even provides more than $6 billion to support Health Savings Accounts outside of Medicare, risking the fragmentation of the broader insurance risk pool.) And in the name of greater cost containment, it encourages the expansion of private plans that have, to date, not saved Medicare money, while creating new budgetary rules that could very well make Medicare less equitable and affordable down the road.
Here is yet some more from this depressing story:
To be sure, politics usually requires compromises. But what’s shameful about the present bill is just how deeply the compromises — or, more accurately, the concessions to knee-jerk beliefs and private interests — undercut the stated goal of the bill: drug coverage for seniors. By our back-of-the envelope calculations, the roughly $400 billion in new spending over the next 10 years (not to mention the $140 billion in new premiums paid by Medicare beneficiaries themselves) will buy only about half as much coverage as a sensibly designed bill could. This is not only because of the subsidies for private health plans and for Health Savings Accounts, but also because of the higher overhead costs of private plans (about five to six times higher than for traditional Medicare) and the 20-to-30-percent higher prices for drugs that seniors will have to pay because Medicare is forbidden from using its bargaining power to negotiate better deals.
Indeed, a significant proportion of Medicare beneficiaries will almost certainly be worse, not better, off under the bill. This includes several million low-income seniors who will lose the generous coverage they now enjoy under state Medicaid programs. It also includes millions who already have pretty good drug coverage through their former employers — coverage which will likely be dropped, despite the bill’s subsidies for employers that retain coverage.
I don’t accept the authors’ implication that our main health care policy goal should be to subsidize seniors, most of whom are relatively wealthy. But it should not be to subsidize pharmaceutical companies either. Read the whole story to learn just how much special interests shaped the final legislation.
Three Oreo Cookies
Obesity rates in the United States have increased dramatically in the past two decades – so much so that manufacturers of everything from clothes to coffins are now super-sizing. But did you know that the entire increase can be explained by three Oreo cookies a day? The trouble is that calories accumulate so holding caloric expenditures constant even a small permanent increase in calories consumed can lead to serious weight gain over long periods of time. Food is getting cheaper and work is becoming more sedentary so it is going to be very difficult to control weight gain. I review some of the recent economic literature on obesity here.
Despite a number of government programs, for example, Swedes continue to get bigger just like everyone else.
For years, this nation of nine million has had the sorts of programs, combining healthy diet and physical exercise, that antiobesity advocates elsewhere in the world dream about. Vending machines in Swedish schools are practically unheard of. TV commercials of any kind aimed at kids under 12 are banned. Schoolchildren as young as eight learn to cook healthy meals. Sports programs are heavily subsidized to get youngsters up and about. But Swedish children are plumping up at alarming rates anyway. The number of kids who are overweight has tripled in the past 15 years — roughly the same rate as in other European countries — to 19% of boys and 15% of girls.
(From the WSJ via Radley Balko.)
I suspect our only real hope is better tasting fat and sugar substitutes. So far I am not too impressed but I do recommend Russel Stover’s low-carb mint patties.
Medicare and Perverse Incentives
Medicare does little to reward service providers for quality improments, and in fact often punishes them. Friday’s New York Times provided a blistering indictment:
By better educating doctors about the most effective pneumonia treatments, Intermountain Health Care, a network of 21 hospitals in Utah and Idaho, says it saves at least 70 lives a year. By giving the right drugs at discharge time to more people with congestive heart failure, Intermountain saves another 300 lives annually and prevents almost 600 additional hospital stays.
But under Medicare, none of these good deeds go unpunished.
Intermountain says its initiatives have cost it millions of dollars in lost hospital admissions and lower Medicare reimbursements. In the mid-90’s, for example, it made an average profit of 9 percent treating pneumonia patients; now, delivering better care, it loses an average of several hundred dollars on each case.
“The health care system is perverse,” said a frustrated Dr. Brent C. James, who leads Intermountain’s efforts to improve quality. “The payments are perverse. It pays us to harm patients, and it punishes us when we don’t.”
Intermountain’s doctors and executives are in a swelling vanguard of critics who say that Medicare’s payment system is fundamentally flawed.
Medicare, the nation’s largest purchaser of health care, pays hospitals and doctors a fixed sum to treat a specific diagnosis or perform a given procedure, regardless of the quality of care they provide. Those who work to improve care are not paid extra, and poor care is frequently rewarded, because it creates the need for more procedures and services.
Does the Bush Medicare bill make any serious attempt to address problems like this? No. Paul Krugman, in his column, described the Medicare bill as “a huge subsidy for drug and insurance companies, coupled with a small benefit for retirees.” If we are to improve America’s health care system, no matter what your political stance, the first order of business is to get incentives working for us, not against us. That fight has yet to begin, nor does it currently have much of a constituency behind it in either political party.
Who are the uninsured?
As the Democratic candidates call for various versions of national health insurance, we will hear a familiar fact many times, namely how many Americans lack medical insurance. According to one estimate, it is over fifteen percent of the population, which amounts to about 43.6 million people.
But who are these people? In reality many of them are immigrants. Here are two simple facts:
Immigrants who arrived between 1994 and 1998 and their children accounted for an astonishing 59 percent or 2.7 million of the growth in the size of the uninsured population since 1993.
The total uninsured population is one-third larger (32.7 million versus 44.3 million) when the 11.6 million persons in immigrant households without insurance are counted.
Hispanics have by far the lowest rates of being insured, here are some visuals. 41 percent of adult Hispanics are uninsured, of course many of these are recent immigrants, Hispanics as a whole account for over 12 percent of national population.
I am all for a liberal immigration policy, but I do not feel we are obliged to offer health insurance to all comers. In fact I suspect that national health insurance would, in the long run, lead to fiscal pressures to limit immigration, thus damaging the health of potential immigrants.
Nor do immigrants rush to buy their own health insurance, in many cases I suspect they would rather send the money back home, where health care crises are likely more severe:
Lack of insurance remains a severe problem even after immigrants have been in the country for many years. In 1998, 37 percent of immigrants who entered in the 1980s still had not acquired health insurance, and 27.2 percent of 1970s immigrants were uninsured.
Many other Americans lack health insurance because they are out of work. True, a good health care system should be robust to macroeconomic disturbances, but with employment and productivity rising, these people do not represent much of a current case for reform.
It also turns out that many of the uninsured are uninsured for only part of the year. According to the CBO, those uninsured for the entire year amount to somewhere between 21 and 31 million, knocking a full 12 million off the original total.
Some of the uninsured are more accurately a counting error:
According to the National Center for Policy Analysis (NCPA), [a] verification question lowered the estimate of the number of uninsured living in households with annual incomes of $75,000 or more by 16 percent. The verification question lowered by 4 percent the number of uninsured living in households with incomes under $25,000.
Many of the uninsured are in fact college students, who either rely on their parents, or are covered under their parents’ policies, read here. One estimate suggests that one out of seven college students lacks insurance, but it is hard to believe that most of these people have no other resources supporting them.
Finally, the uninsured often have good access to medical care. Consider this:
15 million of the uninsured have incomes of $50,000 or more. The fastest-growing population of uninsured has incomes exceeding $75,000. About 14 million are eligible for Medicaid or the State Children’s Health Insurance Plan but are not enrolled.
The “entire year uninsured” receive about half as much care, in dollar-valued terms, as the fully insured. As a last resort, you can always show up at an emergency room and simply demand care. In the year 2001, uninsured Americans received at least $35 billion in health care treatments.
The bottom line: When you put all the pieces together, the crisis of the uninsured is not nearly as bad as it sounds.
Flu Shots II
I won’t scold you again but Robert Bazell writing in Slate reminds us of the positive externality:
Even if spending a week violently sick and bedridden doesn’t worry you, by immunizing yourself you vastly lessen the chances you will spread the virus to some child or older person (family member, friend, or stranger) who might die from it….An experiment in Japan proved that immunizing school-age children could cut deaths in the elderly by many thousands.
…Most appalling of all, only 34 percent of health-care workers got flu shots. The very people who are most at risk themselves and most likely to spread the virus to others are for the most part not getting their shots.
For those afraid of needles, Bazell notes that you can now get a flu mist instead of a shot.
Update on Medicare reform
Several days ago I predicted that the recent Medicare bill would turn out to be largely the prescription drug benefit, with little real institutional reform in the direction of privatization, for better or worse. An article in today’s New York Times provides a closely related argument.
Here is a summary:
The most politically charged feature of the Medicare legislation passed by Congress – its attempt to make the federal Medicare program compete with private managed-care plans – is also the least likely to come to fruition on the seven-year schedule set in the bill, according to health policy experts…Similar plans, the experts say, have failed to find support among patients, doctors and hospitals, or even some insurers. Even people who favor the idea say the potential for trouble this time is formidable…Many people enrolled in Medicare fear that they will end up with less generous benefits in a privately run program…Nor do hospitals and doctors like the idea of health insurers pushing down fees to make a profit for themselves, and health plans have balked at previous projects that threatened to squeeze their profit margins…In addition, many privately run Medicare plans, known as Medicare H.M.O.’s, withdrew from many areas of the country when government payments lagged, forcing millions of patients to scramble to obtain new coverage.
The bill passed by the House and Senate in the last few days calls for six-year demonstration projects in four to six cities, where private health plans would compete with the traditional Medicare program to enroll subscribers by offering a variety of new services with the goal of possibly reducing costs…But four previous attempts at experimenting with competition among Medicare H.M.O.’s were aborted before they began – blocked in Congress after members heard objections from health care providers and elderly voters.
Arguably this kind of “mixed privatization,” with strong public elements, and few real incentives for cost control, was not a good idea in the first place. But in any case it is unlikely to ever see the true light of day.
Get your Flu Shot!
We do not respond to risks rationally. We are scared of Ebola, pesticides, nuclear radiation and terrorists but the flu? Who cares about the flu? You should. In an average year, the flu kills almost as many people as die in auto accidents (36,000 for the flu, 42, 815 for highway accidents in 2002) and this year experts expect some 50-70 thousand flu deaths. True, those over 65 years of age and older are most at risk but thousands of younger people die from the flu every year. A flu shot reduces your chances of death by 50 percent. (Here is more flu info from the CDC.)
Cadaveric vs Live Organ Donation
The basic point is simple – financial incentives for cadaveric donation of organs would save lives and would also reduce the demand for live donation, a costly and difficult procedure. (See my previous posts on this issue here and here). Tyler’s post obscures the basic point by introducing a debate about “a truly free market in organs” by which he means allowing payment for live donors. I won’t be drawn into that debate today, not because it isn’t an interesting issue, but because it is not germane to the issue of financial incentives for cadaveric donation. We should have the latter regardless of our position on the former. Note also that for obvious reasons live donation primarily affects kidneys only and doesn’t reach the issue of how to save the lives of transplant patients who needs hearts, lungs and other organs.
Sleazeball lawyer in a low-cut dress
I am speaking of Erin Brockovich. Sure, I liked the movie but the true story on which it was based was a lie. There was no cancer cluster in Hinkley, no scientific theory of harm, no coverup at the water office (see here for links). Having had one success in Hollywood, Brockovich is now after another this time by fanning hysteria that the kids at Beverly Hills High School (yes, 90210) are getting cancer from a nearby oil well. I smell a movie in the works.
End Phase 3
Harvard neurologist Peter Lansbury argues in the WP that we should end mandatory Phase 3 clinical trials for new pharmaceuticals. Aside from the expense of Phase 3 trials (hundres of millions of dollars) and years of delay he writes that:
There are also scientific reasons to replace Phase 3. The reasoning behind the Phase 3 requirement — that the average efficacy of a drug is relevant to an individual patient — flies in the face of what we now know about drug responsiveness. Very few drugs are effective in all individuals. In fact, most are not effective in large portions of the population, for reasons that we are just beginning to understand.
It’s much easier to get approval for drugs that are marginally effective in, say, half the population than drugs that are very effective in a small fraction of patients. This statistical barrier discourages the pharmaceutical industry from even beginning to attack diseases, such as Parkinson’s, that are likely to have several subtypes, each of which may respond to a different drug. These drugs are the underappreciated casualties of the Phase 3 requirement; they will never be developed because the risk of failure at Phase 3 is simply too great.
Lansbury also recognizes the importance of off-label prescribing and how it flies in the face of FDA power.
Once the FDA has approved a drug based on its effectiveness against one condition, it can be prescribed for any other condition. This practice recognizes that your physician is best equipped to evaluate all the available information and advise whether you could benefit from a particular drug. About 40 to 50 percent of all drug use is for such unapproved, or “off-label,” uses. Some drugs that “failed” in Phase 3 trials for one condition, but were approved for another, are still widely prescribed for the first because physicians agree that the evidence shows they can be effective.
I agree with Lansbury’s analysis and so do a lot of physicians. See my papers Assessing the FDA via the Anomaly of Off-Label Drug Prescriptions and Do Off-Label Drug Practices Argue Against FDA Efficacy Requirements? Testing an Argument by Stuctured Conversations with Experts.
And you think we economists are tough…
Barlow’s method for treating anxiety disorders is surprisingly simple, although its philosophical and clinical implications are anything but. He aims to reduce anxiety not by teaching customary relaxation techniques involving calming mantras or soothing imagery, but by doing just the opposite: forcing the patient to repeatedly face his most dreaded situation, so that, eventually, he becomes accustomed to the sensation of terror. Barlow claims he can rid some people of their symptoms in as little as five to eight days. His treatment promises to be psychotherapy’s ultimate fast track, but while many clinicians praise its well-documented results, others take a dimmer view of what one clinician calls ”torture, plain and simple.”
The economic rationale for this, is, of course, straightforward. Make some form of thought, feeling or behavior more costly, and people will do less of it.
And does it work?
…his success in ameliorating anxiety is by his reckoning as high as 85 percent. David Tolin, the director of the Anxiety Disorders Center at the Institute of Living in Hartford, says: ”Barlow’s program is an ideal toward which other clinicians should strive. It is the most rigorously tested and documented treatment for anxiety. Most practitioners don’t teach his approach because the field of psychology is relatively slow to adapt to evidence-based treatment.” Reid Wilson, a professor of psychiatry at the University of North Carolina School of Medicine and an ardent Barlow supporter, adds that Barlow’s work hasn’t completely caught on because, as he puts it: ”We’re still on the uphill climb. We haven’t had the manpower to train enough people. Only a very small number of clinicians know about this. They don’t understand that relaxation training could actually slow treatment instead of speed it up.”
For the full, and fascinating, story, click here. Here is another article on Barlow. Here is Barlow’s home page.
I don’t have the clinical or medical expertise to evaluate this, but surely it deserves a closer look. The economist, however, should not spring to any quick conclusions. Yes, the “substitution effect” favors a cure, but in the meantime the “income” or “portfolio” effect may drive the individual to very low and possibly counterproductive levels of despair.
By the way, our colleague Bryan Caplan offers this extreme, economistic perspective on mental illness. I think Bryan’s view is crazy; he probably thinks you would be crazy not to read such a short, entertaining polemic.
US Sperm Exports Explode; Canadians Upset
The US is a world leader in sperm exports primarily because sperm banks in the U.S. are run on a for-profit basis. As a result, US sperm is reckoned to be of high quality (we always knew this didn’t we?) particulary because the US version comes with a background on the vitals of the donor. Denmark also exports a lot of sperm because of high standards and demand for that blond, blue-eyed look.
Exports to Canada have increased in recent years because of a scandal involving poorly screened Canadian sperm. Canadians also import a lot of US eggs. The Canadian government, however, is apparently miffed as a new law is being readied that would forbid donations involving a paid donor. The law would not only make paid donation illegal in Canada it would make it illegal to use any paid-for sperm. Canadian couples seeking fertility options will suffer and who will benefit? I cannot think that this law is anything but spiteful and ridiculous. Is paying for sperm an original sin? As with other areas of Canadian medicine (see Tyler’s posts here and here), the rich will now travel to the United States for treatment.
Aside: The Canadian Health Official quoted here is ignorant or disengeneous when she says “We don’t buy or sell blood, or organs or tissues.” In fact, Canada also imports a lot of US blood plasma. Plasma takes longer to donate than straight blood and as a result altruistic donation rates are low and much of the world relies on paid-for US plasma for its life-saving properties. Similarly, donating eggs is not nearly as much fun as donating sperm so altruistic donation of Canadian eggs is unlikely to make-up for restrictions on the import of paid-for US eggs.
Thanks to Eric Crampton for the seminal email.
Suicide and multiple equilibria
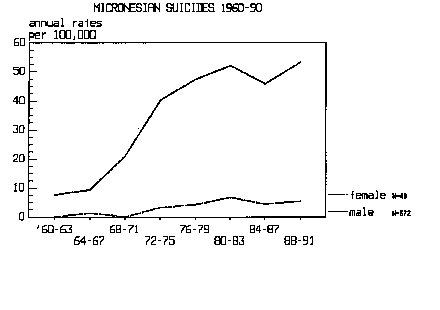
I don’t aim to be the cynical economist that Tyler writes “might suggest social stigma for suicide, rather than forgiveness” but it is frightening how easy it seems to be to jump to the sad equilibrium. The story of suicide among young boys in Micronesia (I recommend Malcolm Gladwell’s The Tipping Point for a discussion but will cite some online material) illustrates how actions and social attitudes reinforce one another. As the action becomes more common, perhaps reaching a “tipping point”, condemnation declines, and the action increases even further. Here, from one of the researchers who first documented the story, is a chilling description of suicide in Micronesia:
As suicide has gained familiarity among youth, the act itself has become increasingly more acceptable or even expected. Suicides appear to acquire a sort of contagious power. One suicide might serve as the model for successive suicides among friends of the first victim. There has been an apparent increase in suicides among very young children, aged 1ï¼-14. Evidently the idea of suicide has become increasingly commonplace and compelling, and young children are now acquiring this idea at earlier ages.
Another of the earlier researchers writes:
Love songs mention suicide, youths discuss the subject openly among themselves and at times make suicide pacts with one another, and youngsters express admiration of those who have taken their own lives and are mourned so terribly by their families and friends. What is even more shocking, however, is that a number of adults in our communities seem to share the belief that these young people have died altruistic and even heroic deaths. If the majority of Micronesians really believe that suicide is an honorable option, then this paper is thoroughly useless and all of us had better resign ourselves to continuing high rates of suicide in the future. Young people, after all, are very quick in sensing the basic values of their elders. If they get the impression that we ourselves honor suicide, then they will be only too happy to oblige by hanging themselves.
Note that one could tell similar stories in the United States about divorce, having children out of wedlock, welfare dependence etc. (also teenage suicide at a local level).
Here is a graph of suicide rates in Micronesia indicating a massive increase in a few short years in the early 1970s. The tipping theory generates credence when we note that virtually all the suicides take a similar, ritualistic form involving hanging.
Dalkon Shield, Silicone Breast Implants, Fen-Phen
A bill to move class action lawsuits out of the state courts and into federal courts narrowly failed in the Senate. Senator Tom Daaschle, explained his opposition to the bill this way, “It is the Dalkon shield, it is silicone breast implants, it is fen/phen.”
Good list. Wrong conclusion. The A.H. Robins Co. was driven into bankruptcy and forced to pay 3 billion dollars in damages but the Dalkon shield has been shown to be effective and safe. Silicone breast implants have been reviewed in studies by the AMA, the Institute of Medicine, the Canadians, the French, the British and others. All conclude that there are no unusual problems with the implants (any surgery has risks of course). The FDA will probably soon allow the implants back onto the market but in the meantime Dow-Corning has been driven into bankruptcy and tens of millions of dollars have been spent on lawsuits. Fen/Phen does looks like a serious health risk but tort law had nothing to do with removing the product from the marketplace. (Moreover, the issue is complicated. Only the Fen in Fen/Phen looks dangerous and that was approved in 1973).