The Great Barrington Plan: Would Focused Protection Have Worked?
A key part of The Great Barrington Declaration was the idea of focused protection, “allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk.” This was a reasonable idea and consistent with past practices as recommended by epidemiologists. In a new paper, COVID in the Nursing Homes: The US Experience, my co-author Markus Bjoerkheim and I ask whether focused protection could have worked.
Nursing homes were the epicenter of the pandemic. Even though only about 1.3 million people live in nursing homes at a point in time, the death toll in nursing homes accounted for almost 30 per cent of total Covid-19 deaths in the US during 2020. Thus we asked whether focusing protection on the nursing homes was possible. One way of evaluating focused protection is to see whether any type of nursing homes were better than others. In other words, what can we learn from best practices?
The Centers for Medicaire and Medicaid Services (CMS) has a Five-Star Rating system for nursing homes. The rating system is based on comprehensive data from annual health inspections, staff payrolls, and clinical quality measures from quarterly Minimum Data Set assessments. The rating system has been validated against other measures of quality, such as mortality and hospital readmissions. The ratings are pre-pandemic ratings. Thus, the question to ask is whether higher-quality homes had better Covid-19 outcomes? The answer? No.
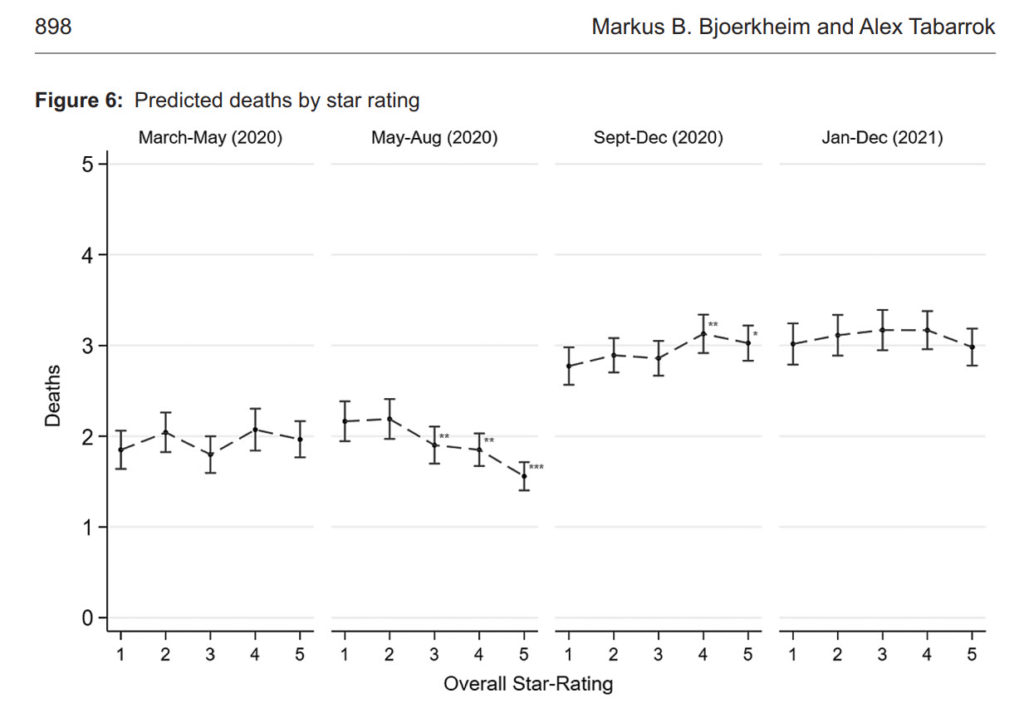
The following figure shows predicted deaths by 5-star rating. There is no systematic relationship between nursing homes rating and COVID deaths. (In the figure, we control for factors outside of a nursing homes control, such as case prevalence in the local community. But even if you don’t control for other factors there is little to no relationship. See the paper for more.) Case prevalence in the community not nursing home quality determined death rates.
More generally, we do some exploratory data analysis to see whether there were any “islands of protection” in the sea of COVID and the answer is basically no. Some facilities did more rapid tests and that was good but surprisingly (to us) the numbers of rapid tests needed to scale nationally and make a substantial difference in nursing home deaths was far out of sample and below realistic levels.
Finally, keep in mind that the United States did focused protection. Visits to nursing homes were stopped and residents and staff were tested to a high degree. What the US did was focused protection and lockdowns and masking and we still we had a tremendous death toll in the nursing homes. Focused protection without community controls would have led to more deaths, both in the nursing homes and in the larger community. Whether that would have been a reasonable tradeoff is another question but there is no evidence that we could have lifted community controls and also better protected the nursing homes. Indeed, as I pointed out at the time, lifting community controls would have made it much more difficult to protect the nursing homes.