Category: Medicine
Repeal the employer mandate altogether
I agree with Ezra Klein, who writes:
Delaying Obamacare’s employer mandate is the right thing to do. Frankly, eliminating it — or at least utterly overhauling it — is probably the right thing to do. But the administration executing a regulatory end-run around Congress is not the right way to do it.
Ezra notes:
– By imposing a tax on employers for hiring people from low- and moderate-income families who would qualify for subsidies in the new health insurance exchanges, it would discourage firms from hiring such individuals and would favor the hiring — for the same jobs — of people who don’t qualify for subsidies (primarily people from families at higher income levels).
– It would provide an incentive for employers to convert full-time workers (i.e., workers employed at least 30 hours per week) to part-time workers.
– It would place significant new administrative burdens and costs on employers.
By tying the penalties to how many full-time workers an employer has, and how many of them qualify for subsidies, the mandate gives employers a reason to have fewer full-time workers, and fewer low-income workers.
We can only hope that repeal of this one part of the law is what the Obama Administration actually has in mind, though as Ezra notes Congress is not currently in a cooperative frame of mind. Still, this way it has a chance of serious reexamination after the 2014 elections.
Evan Soltas offers relevant comment on how this will change implementation in the short-run, namely that it puts more burden on the exchanges. Sarah Kliff comments on the politics, a very good post. Here is one good quotation from a source: “Politically, it won’t get easier a year from now, it will get harder,” he said. “You’ve given the employer community a sense of confidence that maybe they can kill this. If I were an employer, I would smell blood in the water.”
My view is you don’t serve up a delay and PR disaster like this, on such a sensitive political issue, unless you really wish to derail the entire provision.
*World War Z*
I was surprised how serious a movie it is and also by how deeply politically incorrect it is, including on “third rail” issues such as immigration, ethnic conflict, North Korean totalitarianism, American urban decay as exemplified by Newark, gun control, Latino-Black relations, songs of peace, and the Middle East. Here is one (incomplete) discussion of the Middle East angle, from the AP, republished in el-Arabiya (here is a more detailed but less responsible take on the matter, by a sociology professor and Israeli, spoilers throughout).
The movie is set up to show sympathy for the “Spartan” regimes and to have a message which is deeply historically pessimistic and might broadly be called Old School Conservative, informed by the debates on martial virtue from pre-Christian antiquity. But they recut the final segment of the movie and changed the ending altogether, presumably because post-Christian test audiences and film executives didn’t like it. Here is one discussion of the originally planned finale. It sounds good to me. The actual movie as it was released reverts to a Christian ending of sorts. My preferred denouement would have relied on the idea of an asymptomatic carrier or two, go see it and figure out the rest yourself.
By the way, for all the chances taken by the film makers, they were unwilling to offend the government of China (see the first link), in part because you cannot trick them easily with subtle, veiled references. Such tomfoolery works only on Americans — critics included — which I suppose suggests a lesson of its own.
Here is a Times of Israel review of the movie, interesting throughout, and it notes that the Israel scenes are simply translated to “the Middle East” for Turkish audiences.
A good film, I liked it. How many other movies offer commentary on Thucydides, Exodus, Gush-Shalom, Lawrence Dennis, and George Romero, all rolled into one?
Amish arbitrage fact of the day
Eight percent of one sample (n = 112) of Lancaster county Amish have sought medical care in Mexico.
That is from Donald B. Kraybill, Karen M. Johnson-Weiner, and Steven M. Nolt, The Amish, which is an excellent social scientific look at what we outsiders know about Amish communities.
I also learned that the Amish strongly frown on home schooling of children and consider it possible grounds for excommunication. The requirement to use the internet has pushed many Amish out of public school systems, and the Amish are experts at making apprenticeship systems work. Inequality of wealth seems to be rising among the Amish.
The Great Canadian Sperm Shortage
As I was researching yesterday’s post on The Oocyte Cartel I came across an old MR post from 2003 on plans in Canada to restrict the import of American sperm:
The US is a world leader in sperm exports primarily because sperm banks in the U.S. are run on a for-profit basis. As a result, US sperm is reckoned to be of high quality particularly because the US version comes with a background on the vitals of the donor. Denmark also exports a lot of sperm because of high standards and demand for that blond, blue-eyed look.
Exports to Canada have increased in recent years because of a scandal involving poorly screened Canadian sperm. Canadians also import a lot of US eggs. The Canadian government, however, is apparently miffed as a new law is being readied that would forbid donations involving a paid donor. The law would not only make paid donation illegal in Canada it would make it illegal to use any paid-for sperm. Canadian couples seeking fertility options will suffer and who will benefit? I cannot think that this law is anything but spiteful and ridiculous. Is paying for sperm an original sin?
So what happened? In 2004, Canada made it a criminal offense to compensate sperm and egg donors. Loyal readers will not be surprised by the results (as of 2011)
…currently, in the entire country, there are only 35 active sperm donors. Over the last decade, our government has made its donation system so thoroughly unappealing that this ubiquitous fluid is almost impossible to obtain through official channels. There is a single operating sperm bank in all of Canada.
…If 35 national donors is an ugly statistic for the most removed observer, it’s especially devastating for the women and couples who have come to rely on our lone sperm bank in order to have a child.
Ironically, it’s been easier to prevent payments to Canadian donors than it has been to police sperm and egg imports because it is still technically legal to use paid-for sperm just not to buy sperm. As a result, the importation of US sperm has increased:
Patients here obtain more than 90% of semen from the United States, and the federal government appears to turn a blind eye to the fact they buy it from mostly for-profit sperm banks — a criminal offence in this country.
Addendum: Some readers may find all this talk of sex and sperm to be risque but do remember this is a family-friendly blog.
The Oocyte Cartel
The Society for Assisted Reproductive Technology (SART) represents more than 85 percent of the assisted reproduction industry. SART requires that its members work only with agencies that limit compensation to egg-donors to around $5000 or a maximum of $10,000 (figures decided upon by the ethics committee of an affiliated organization, The American Society for Reproductive Medicine (ASRM)). In other words, ASRM-SART acts as a buyer’s cartel.
In 2011, Lindsay Kamakahi launched a class action suit against ASRM-SART challenging their horizontal price-fixing agreement as per se illegal under the Sherman Antitrust Act. ASRM-SART tried to have the case dismissed but a judge recently denied the dismissal in the process making it clear that the plaintiffs have a good case.
ASRM-SART argue that their maximum price is really about protecting women and that compensation “should not be so excessive as to constitute undue inducement.” Egg donation does involve extensive screening, time and some health risks. One would think, however, that the proper response for those interested in protecting women would be to ensure that the women are fully informed and that they are paid high wages not low wages.
The paternalistic policy of the ASRM-SART especially rankles because it applies only to women, sperm donations are not regulated. Of course, sperm donation isn’t risky but we also don’t see laws limiting the wages of miners to protect miners (mostly men) from “undue inducement.” The societal expectation seems to be that men are appropriately motivated by self-interest but women may be appropriately motivated only by altruism.
I am in agreement with Kimberly D. Krawiec who writes in her excellent paper Sunny Samaritans and Egomaniacs: Price-Fixing in the Gamete Market:
It is ASRM’s paternalistic and misguided attempts to control oocyte donor compensation through the same type of professional guidelines that courts have rejected when employed by engineers, lawyers, dentists, and doctors that should raise an ethical red flag.
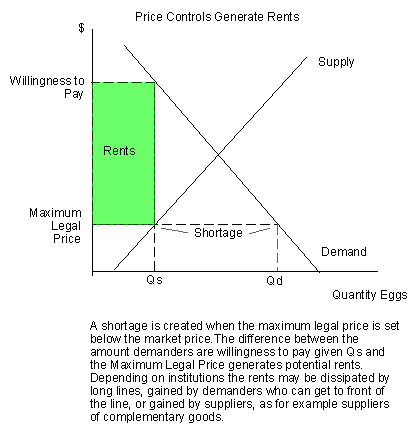 ASRM-SART surely believe that they are doing good but I think it no accident that they also do well from a policy that reduces the price of their inputs. A price controlled below the market price generates rents. In the traditional analysis, the rents are dissipated away by long-lines, a form of rent seeking (see Modern Principles–first edition now a bargain!). It’s also possible, however, for suppliers to grab up the rents, especially suppliers of complementary goods.
ASRM-SART surely believe that they are doing good but I think it no accident that they also do well from a policy that reduces the price of their inputs. A price controlled below the market price generates rents. In the traditional analysis, the rents are dissipated away by long-lines, a form of rent seeking (see Modern Principles–first edition now a bargain!). It’s also possible, however, for suppliers to grab up the rents, especially suppliers of complementary goods.
For example, it’s often been pointed out that in the organ donor market the hospitals, surgeons and executives all get paid and paid well; the only person not getting paid is the person who provides the transplant organ. But we can say more–one of the reasons the hospitals, surgeons and executives get paid well is precisely that the donor is not paid. The shortage created by the price control drives the demander’s willingness to pay upward and some of the difference between the willingness to pay and the maximum legal price is captured by the suppliers of complementary inputs. How do we know? In the 1990s, entry into the transplant business grew much faster than did the supply of transplant organs. In fact, transplants were so profitable there was a rush to transplant that increased the number of centers but drove down center volume thereby reducing patient survival rates.
Similarly, by limiting egg-supply the suppliers of assisted reproductive services may be able to increase their share of the total gains from trade.
Although ASRM-SART may profit from restricting donor compensation there is another issue at large, the repugnance constraint. The repugnance and disgust centers of the brain are old and deep and often revolve around issues of body integrity, body products, hygiene, sex and death. Birth treads uneasily in many of these waters already and egg donation adds to this volatile mix issues of gender, personhood, identity and genetics all of which prime for a repugnance storm. The plaintiff’s case is sound but if the antitrust laws prevent ASRM-SART from limiting prices–or saying that they limit prices–and if egg donation were to become even more of a market in everything might there not be a backlash and an outright ban on compensated donors, as is the case in many other countries and for transplant organs in this country? I hope not but it is a real possibility.
The ban on compensated transplant organ donation has led to hundreds of thousands of excess deaths. A ban on compensated sperm and egg donation would lead to a dearth of lives.
*Confessions of a Sociopath*
I suspect nothing in this book can be trusted. Still, it is one of the more stimulating reads of the year, though I have to be careful not to draw serious inferences from it. Does its possible fictionality make it easier to create so many interesting passages?:
I can seem amazingly prescient and insightful, to the point that people proclaim that no one else has ever understood them as well as I do. But the truth is far more complex and hinges on the meaning of understanding. In a way, I don’t understand them at all. I can only make predictions based on the past behavior they’ve exhibited to me, the same way computers determine whether you’re a bad credit risk based on millions of data points. I am the ultimate empiricist, and not by choice.
The author argues that sociopaths are often very smart, have a lot of natural cognitive advantages in manipulating data, and are frequently sought out as friends for their ability to appeal to others. It is claimed that, ceteris paribus, we will stick with the sociopath buddies, as we are quite ready to use sociopaths to suit our own ends, justly or not. It is claimed that for all of their flaws, many but not all sociopaths are capable of understanding what is in essence the contractarian case for being moral — rational self-interest — and sticking with it. Citing some research in the area (pdf), the author speculates that sociopaths may have an “attention bottleneck,” so they do not receive the cognitive emotional and moral feedback which others do, unless they decide very consciously to focus on a potential emotion. For sociopaths, top down processing of emotions is not automatic.
We even learn that (supposedly) sociopaths are often infovores. It seems many but not all sociopaths are relatively conscientious, and the author of this book (supposedly) teaches Sunday school and tithes ten percent to the church. It just so happens sociopaths sometimes think about killing or destroying other people, without feeling much in the way of remorse.
I can also recommend this book as an absorbing memoir of a law professor and also of a Mormon outlier. It is written at a high level of intelligence, and it details how to get good legal teaching evaluations, how to please colleagues, how to evade Mormon proscriptions on sex before marriage, and it offers an interesting hypothesis as to why sociopaths tend to be more sexually flexible than the average person (hint: think more systematically about what abnormal or weakened top-down processing of emotions might mean in other spheres of life).
The author argues that sociopaths can do what two generations of econometricians have only barely managed, namely to defeat the efficient markets hypothesis and earn systematically super-normal returns. What does it say about me that I find this the least plausible claim in the entire book?
Here is a useful New York Times review. Here is the author’s blog, which is about being a sociopath, or about pretending to be a sociopath, or perhaps both. Here is the book on Amazon and note how many readers hated it. I say they just don’t like sociopaths.
One hypothesis is that this book is a stunt, designed as an experiment in one’s ability to erase or conceal an on-line identity, although I would think a major publisher (Crown) is not up for such tricks these days. An alternative is that a sociopath — not the one portrayed in the book — is trying to frame an innocent person as the author of the book (some trackable identity clues are left), noting that the book itself discusses at length plans to destroy others for various (non-justified) reasons. Or is it a Straussian critique of the Mormon Church for (supposedly) encouraging sociopathic-related character traits in its non-sociopath members? Or all of the above?
{kind=link}
You will note that the book’s opening diagnosis comes from an actual clinical psychologist in the area, and the Crown legal department would have no interest in misrepresenting him in this manner. So the default hypothesis has to be that this book represents some version of the truth, at least as seen through the author’s eyes.
Some version of the author, wearing a blonde wig it seems, appeared on the Dr. Phil show, to the scorn of Phil I might add.
I cannot evaluate the scientific claims in this book, and would I trust the literature on sociopaths anyway, given that the author claims it is subject to the severe selection bias of having more access to the sociopathic losers and criminals? (I buy this argument, by the way.) It did occur to me however, that for the rehabilitation of sociopaths, whether through books or other means, perhaps they should consider…a rebranding exercise? But wait, “Sorry, I could not find synonyms for ‘sociopath’.”
If nothing else, this book will wake you up as to how little you (probably) know about sociopaths.
Which market segment is being targeted by Kaiser in California?
Megan McArdle updates us:
Kaiser Permanente is one of the places that always gets cited as a model by health care reformers. It’s the biggest insurer in California, using a model that ended up being the basis for the HMO revolution. Kaiser owns its own hospitals, pays its doctors a salary, and provides the “continuum of care” that everyone says they want from our fragmented health care system–and does it at a reasonable price. So it’s a bit surprising to see the LA Times report that this model citizen submitted some of the highest bids for California’s health care exchanges.
…California is headed for two-tier service on the Exchanges. The carriage trade will head for full-service networks like Kaiser, with full access to the whole network of doctors and hospitals. The price conscious buyers–likely to be a sizeable majority–will crowd into plans with restrictive networks. And those networks will be very, very crowded. Effectively, they may end up as quasi-catastrophic insurance, simply because it will be difficult to actually access care outside of the emergency room.
Lower down the income scale, the new Medicaid patients–about half the expected additional coverage in states like California–will be similarly crowded, simply because Medicaid’s low reimbursement rates make doctors reluctant to take it.
Note that, for reasons explained in the post, this may not apply outside of California in every other state.
I am proud of the Dotchka
Yana flew yesterday from Newark airport and will be arriving in Mumbai shortly, heading in a few days to live in Bangalore. She will be working with Forus Health to decrease preventable blindness among India’s poor, in part by aiding with their distribution of an affordable screening device.
Her indiegogo project is here, which also describes her trip and mission. I hope to visit later in the year. And I expect her to come back knowing three or four more languages.
No Patents on Genes
The Supreme Court ruled unanimously yesterday in Association of Molecular Pathology v. Myriad Genetics that a gene, such as BRCA1 or BRCA2, does not qualify for a patent. The fact that Myriad isolated the DNA is not enough to distinguish it from its in situ counterpart as the information it contains is the same. However, cDNA, a version of the gene that has been stripped of non-coding sequences is subject to patent.
 With this ruling the price of most of Myriad’s tests will fall as competition enters the market (the BRACAnalysis tests are actually a number of different tests, as I read the technical specifications, only some of these depend on cDNA. The markets appeared to have been initially confused about this.). Even more importantly, the Myriad patents were broad and they prevented researchers from freely studying the BRCA1 and BRCA2 genes, from improving the tests or from developing additional applications. The giants demanded payment (video) from those who would stand on their shoulders. I think the restrictions retarded progress–as have similar restrictions–to an extent that made the patents difficult to justify.
With this ruling the price of most of Myriad’s tests will fall as competition enters the market (the BRACAnalysis tests are actually a number of different tests, as I read the technical specifications, only some of these depend on cDNA. The markets appeared to have been initially confused about this.). Even more importantly, the Myriad patents were broad and they prevented researchers from freely studying the BRCA1 and BRCA2 genes, from improving the tests or from developing additional applications. The giants demanded payment (video) from those who would stand on their shoulders. I think the restrictions retarded progress–as have similar restrictions–to an extent that made the patents difficult to justify.
Although I am broadly in agreement with the ruling, it’s also clear that the limited flexibility of patent law–you get a 20-year patent or nothing–and the fact that patent law is not based on patent theory (pdf) greatly hampers the ability to tailor patent law optimally. The ruling, for example, says that a firm can’t patent a gene that it discovers but it can patent the cDNA that it develops. It’s the discovery, however, that’s expensive. The development of cDNA is today a trivial step. Thus, you can patent the trivial step but not the giant leap.
You might think that the law draws a bright line between discoveries which cannot be patented and inventions which can but that’s not correct. Discoveries can be patented and the ruling goes out of its way to push back against the view that they can’t. The ruling correctly notes that a “considerable danger” is that patents on basic ideas and tools would “inhibit future innovation”. Yet the law makes no mention of these considerations and the court provides no guidance on implementation.
Coherent or not, the recent patent cases do indicate that the SC is no longer acceding to the United States Court of Appeals for the Federal Circuit–they are reestablishing control and pushing back in the right direction on the Tabarrok curve.
A New FDA for the Age of Personalized, Molecular Medicine
In a brilliant new paper (pdf) (html) Peter Huber draws upon molecular biology, network analysis and Bayesian statistics to make some very important recommendations about FDA policy. Consider the following drugs (my list):
Drug A helps half of those to whom it is prescribed but it causes very serious liver damage in the other half. Drug B works well at some times but when administered at other times it accelerates the disease. Drug C fails to show any effect when tested against a placebo but it does seem to work in practice when administered as part of a treatment regime.
Which of these drugs should be approved and which rejected? The answer is that all of them should be approved; that is, all of them should be approved if we can target each drug to the right patient at the right time and with the right combination of other drugs. Huber argues that Bayesian adaptive testing, with molecular biology and network analysis providing priors, can determine which patients should get which drugs when and in what combinations. But we can only develop the data to target drugs if the drugs are actually approved and available in the field. The current FDA testing regime, however, is not built for adaptive testing in the field.
The current regime was built during a time of pervasive ignorance when the best we could do was throw a drug and a placebo against a randomized population and then count noses. Randomized controlled trials are critical, of course, but in a world of limited resources they fail when confronted by the curse of dimensionality. Patients are heterogeneous and so are diseases. Each patient is a unique, dynamic system and at the molecular level diseases are heterogeneous even when symptoms are not. In just the last few years we have expanded breast cancer into first four and now ten different types of cancer and the subdivision is likely to continue as knowledge expands. Match heterogeneous patients against heterogeneous diseases and the result is a high dimension system that cannot be well navigated with expensive, randomized controlled trials. As a result, the FDA ends up throwing out many drugs that could do good:
Given what we now know about the biochemical complexity and diversity of the environments in which drugs operate, the unresolved question at the end of many failed clinical trials is whether it was the drug that failed or the FDA-approved script. It’s all too easy for a bad script to make a good drug look awful. The disease, as clinically defined, is, in fact, a cluster of many distinct diseases: a coalition of nine biochemical minorities, each with a slightly different form of the disease, vetoes the drug that would help the tenth. Or a biochemical majority vetoes the drug that would help a minority. Or the good drug or cocktail fails because the disease’s biochemistry changes quickly but at different rates in different patients, and to remain effective, treatments have to be changed in tandem; but the clinical trial is set to continue for some fixed period that doesn’t align with the dynamics of the disease in enough patients
Or side effects in a biochemical minority veto a drug or cocktail that works well for the majority. Some cocktail cures that we need may well be composed of drugs that can’t deliver any useful clinical effects until combined in complex ways. Getting that kind of medicine through today’s FDA would be, for all practical purposes, impossible.
The alternative to the FDA process is large collections of data on patient biomarkers, diseases and symptoms all evaluated on the fly by Bayesian engines that improve over time as more data is gathered. The problem is that the FDA is still locked in an old mindset when it refuses to permit any drugs that are not “safe and effective” despite the fact that these terms can only be defined for a large population by doing violence to heterogeneity. Safe and effective, moreover, makes sense only when physicians are assumed to be following simple, A to B, drug to disease, prescribing rules and not when they are targeting treatments based on deep, contextual knowledge that is continually evolving:
In a world with molecular medicine and mass heterogeneity the FDA’s role will change from the yes-no single rule that fits no one to being a certifier of biochemical pathways:
By allowing broader use of the drug by unblinded doctors, accelerated approval based on molecular or modest—and perhaps only temporary—clinical benefits launches the process that allows more doctors to work out the rest of the biomarker science and spurs the development of additional drugs. The FDA’s focus shifts from licensing drugs, one by one, to regulating a process that develops the integrated drug-patient science to arrive at complex, often multidrug, prescription protocols that can beat biochemically complex diseases.
…As others take charge of judging when it is in a patient’s best interest to start tinkering with his own molecular chemistry, the FDA will be left with a narrower task—one much more firmly grounded in solid science. So far as efficacy is concerned, the FDA will verify the drug’s ability to perform a specific biochemical task in various precisely defined molecular environments. It will evaluate drugs not as cures but as potential tools to be picked off the shelf and used carefully but flexibly, down at the molecular level, where the surgeon’s scalpels and sutures can’t reach.
In an important section, Huber notes that some of the biggest successes of the drug system in recent years occurred precisely because the standard FDA system was implicitly bypassed by orphan drug approval, accelerated approval and off-label prescribing (see also The Anomaly of Off-Label Prescribing).
But for these three major licensing loopholes, millions of people alive today would have died in the 1990s. Almost all the early HIV- and AIDS-related drugs—thalidomide among them—were designated as orphans. Most were rushed through the FDA under the accelerated-approval rule. Many were widely prescribed off-label. Oncology is the other field in which the orphanage, accelerated approval, and off-label prescription have already played a large role. Between 1992 and 2010, the rule accelerated patient access to 35 cancer drugs used in 47 new treatments. For the 26 that had completed conventional followup trials by the end of that period, the median acceleration time was almost four years.
Together, HIV and some cancers have also gone on to demonstrate what must replace the binary, yes/ no licensing calls and the preposterously out-of-date Washington-approved label in the realm of complex molecular medicine.
Huber’s paper has a foreword by Andrew C. von Eschenbach, former commissioner of the FDA, who concludes:
For precision medicine to flourish, Congress must explicitly empower the agency to embrace new tools, delegate other authorities to the NIH and/or patient-led organizations, and create a legal framework that protects companies from lawsuits to encourage the intensive data mining that will be required to evaluate medicines effectively in the postmarket setting. Last but not least, Congress will also have to create a mechanism for holding the agency accountable for producing the desired outcomes.
From the comments
Rahul writes:
Just for the heck of it, I tried an alternative list:
1. Ramp up drastically the training output of new doctors and nurses: More med schools, larger intakes per school, elimination of 4 years of pre-med university etc. More med school student scholarships and subsidies?
2.Massively expand other lower tiers of the medical system: Physicians assistants, Nurse Practitioners etc.
3. Liberalize drug imports both commercial and personal. Allow direct import of any FDA-licensed drug sold in equivalent nations (western EU / Canada etc.). Mostly ignore Big Pharma’s opinions in this context.
4. Fully recognize all medical degrees from similarly developed nations (e.g. Canada / UK / Japan / Australia etc.) to the point that doctors from these nations can register and practice almost instantly in the US. Provide an almost limitless immigration quota for doctors from western nations. Even better, aggressively recruit doctors from abroad. Mostly ignore APA’s opinions in this context.
5. Allow and encourage Medicare / Insurance procedures to be carried out abroad where cheaper locales (Mexico? Canada? Argentina? ) exist. Incentivize recipients using these options. Premium rebates? Encourage private insurers to offer plans that economize on major procedures by treating abroad.
Options for health care coverage reform
This topic has been reconsidered much as of late, so I thought I would do a summary post on some of the possible options. I suspect I have covered all or most of this ground in 2009 or so, but here goes:
1. Universal health insurance vouchers on exchanges, with means-tested subsidies and also a mandate. The logic of this can work just fine, but it is quite expensive as it would exist in the United States and we end up spending too much on health care. Over time it would be accompanied by say a five percent VAT.
2. Single payer systems. I don’t want to repeat the usual debates, but perhaps we can agree single payer won’t come anytime soon in the United States. I also think they work least well in the land of medical innovation, and best in small countries such as New Zealand, but that consideration doesn’t even rise to the fore here.
3. The Singapore system, involving single payer for catastrophic expenses and health savings accounts for smaller expenditures. To varying degrees you can combine this with forced savings for the HSAs and price controls on service provision, both of which you will find in Singapore. Where “catastrophic” starts can vary as well. This is my first choice, although if you wish to dismiss it as “utopian” for the United States you have a point. I’ll get back to that.
4. One particular path for how ACA could evolve into a (relatively inefficient) form of a Singapore system. Imagine that the mandate becomes fairly narrow with time, while at the catastrophic end insurance companies evolve into (inefficient) public utilities. Health savings accounts are reintroduced through new legislation, perhaps under a Republican administration, and can be supplemented with cash transfers when desired. Here is one discussion of that path.
5. The mandate and subsidized exchanges under Obamacare prove unworkable and eventually they are abandoned either partially or in full, or in some states but not others. Their place is taken by a Medicaid expansion. Coverage is not universal, though it is higher than pre-ACA, and of course coverage under the status quo is not going to be universal either.
6. The status quo of Obamacare.
7. More managed care. We should remove the legal restrictions and barriers which penalized managed care in the first place, as it is a feasible and desirable means of bending the health care cost curve. You will note that this option is not a strictly rival alternative to 1-6, but rather can be combined with them in varying degrees. Still, it seems appropriate to list it as an option.
Now, if I am allowed to be utopian, I favor #3 over the status quo. If I am asked to be less utopian, I see #4, #5, and #7 as some of the better versions of what ACA could evolve into. I would not predict that those options come to pass, nor would I say those options are better than the rather unrealistic version of ACA as envisioned by its proponents, but I think they follow from the dictates of reality as the better options on the table, #3 aside of course. And I do not feel I am being utopian in holding them as alternatives to the status quo. They are not so far away from the status quo in the policy space.
I don’t think ACA in its current form is stable. Too many moving parts, too many margins of danger, too many jerry-rigged incentives, too many “it worked OK in Massachusetts so it has to work at the national level even if it doesn’t appear to be maximizing” requirements, and too little recognition that the whole system is poorly geared for a world of stagnant median wages and rising inequality. The higher is inequality and the lower are lower-tier wages, the harder it is to guarantee near-equal consumption of health care through employment institutions. The greatest single danger to ACA is eventual massive employer-shedding of health care obligations, penalties or no, which at best evolves us into #1, which I do not favor. On top of that there is state shedding of Medicaid obligations, which again pushes us into #1. Most generally, the national health care systems which work are much more consolidated in nature than is the U.S. status quo.
It is a Denkfehler when people write “you don’t have an alternative to ACA” or “the Republicans don’t have a health care plan,” and so on. You can take such pronouncements as leading indicators that ACA is not going well. #3 aside, you can take the relevant alternatives as a mix of #4, #5, and #7. Those are not so much alternatives “given by the Republicans (or whoever else),” as much as they are given by reality. I don’t see “ACA as envisioned by its propnents” as on the table either, so in this sense it is also the Democrats who don’t have an actual health care plan.
I view the real choice before us as #1 vs. some mix of #4, #5, and #7. And in that setting I do not favor #1 and I still can dream of and advocate #3.
Addendum: Here is my earlier post on how to debate health care policy. Let’s see how many of its strictures you all violate.
Should states jump on the Medicaid expansion bandwagon?
Carter C. Price and Christine Eibner have a new study in Health Affairs suggesting a definite “yes,” and I have seen this piece endorsed numerous times in the blogosphere and on Twitter. I do understand that part of their argument is a normative one, given the desire to expand insurance coverage for the currently uninsured. But they and their endorsers also seem to be making a state-level financial prudence argument, as if there were no possible reason for a state not to expand participation behind sheer ideological stubbornness. On that matter I don’t think they have pondered the problem deeply enough and they fail an intellectual Turing test.
Let’s start with a simple observation, namely that a Republican may win the next Presidential election. There is also quite a good chance that such a victory would be accompanied by a Republican Senate (and House), given the distribution of vulnerable seats. That means a very real chance that the federal government will scale back its commitment to Medicaid expansion, for better or worse. States don’t want to be left holding the bag, and governors know it is hard to take back benefits once granted.
I often interpret the Republicans as operating in a “they don’t really mean what they say” mode, but on Medicaid I think they basically do mean it and we already can see some of the demonstrated preference evidence. Furthermore a new Republican President would face very real pressure to “repeal Obamacare,” yet we all know that the “three-legged stool” centered around the mandate is hard to undo selectively. That ups the chance Medicaid will be the target and much of the rest will be relabeled (“repealed,” in the press release) but in some manner kept in place in its essentials.
Another possibility is that a Republican administration would somehow restructure the deal to, in some way, favor the holdout red states, relative to the deal already on the table. (Why not reward your supporters?) That increases the prospective return to being a holdout red state.
On top of all this, there is option value. The chance to jump on the Medicaid expansion bandwagon won’t go away tomorrow. Even if the cost-benefit ratio > 1, you still might want to play wait and see. There is even a chance that in the meantime you are somehow offered a better deal yet.
Now if someone wants to argue that, given these considerations, Medicaid expansion still makes financial sense for a state, fine, I would be keen to read such an analysis. But that is not what I am seeing. The Price and Eibner piece doesn’t analyze these considerations or even bring up most of them. Governors are not stupid, or their chiefs of staff are not stupid, and many governors are far less ideological than they let on. They are politicians. And they are politicians who understand that the federal government is not to be trusted and yes if you wish you really can blame that on the Republicans, or indeed on any prospective switch of power. That is why we are not seeing more states do the Medicaid expansion. In the meantime, the debate needs to catch up to the reality.
Is there ACA rate shock in California?
I wasn’t going to weigh in on this, but enough of you have asked me what I think of Avik Roy’s claim that California insurance premiums, under ACA, will go up 64% to 146%. Let me start by telling you this: based on a reading of the secondary commentary, I cannot tell you how much rates in California will be going up (and my original inclination was not to blog it for this reason).
Still, the question having been raised, let’s go back in time. In 2009, the CBO wrote (pdf):
CBO and JCT estimate that the average premium per person covered (including dependents) for new nongroup policies would be about 10 percent to 13 percent higher in 2016 than the average premium for nongroup coverage in that same year under current law.
About half of those enrollees would receive government subsidies that would reduce their costs well below the premiums that would be charged for such policies under current law.
If you read their subsequent discussion, it seems fairly clear to me they are not averaging “higher premia for those still getting insurance” with “a price decline from infinity, for those who couldn’t get any insurance in the pre-ACA days,” in some kind of complicated index number fashion. They are talking about price increases on already-existing policies and what kind of continuation one can expect.
I will treat this as the canonical estimate, and stipulate that we will have had “rate shock” if the percentage increases are three times higher than had been forecast by the CBO.
You will note that these higher rates still may be an efficient form of lump sum taxation, or they may be unsustainable price hikes which cause the mandate to unravel (read Will on this point) by encouraging non-participation, or perhaps a bit of both. Megan McArdle considers some public choice implications of unpopular and unexpected high rates.
In 2009, you will find a claim by Jonathan Gruber:
What we know for sure the bill will do is that it will lower the cost of buying non-group health insurance.
Maybe he had in mind an index-number weighting where the “price decline from infinity” weighs heavily in the calculation and in that sense such a claim can always be true if even one person receives extra coverage. Still, I am more likely to call it a misspoken sentence, a Denkfehler, an excess enthusiasm, and most of all a highly inexact way of describing the issue no matter what is the truth. It was always the case that the median and modal individual premium was likely to go up, even with full political cooperation from the Republicans. After all, that is part of the “efficient lump sum taxation” idea behind the use of the mandate in the first place. And yes I do understand that a competitiveness effect and a transparency effect still may push prices down but that is not the way I would bet it and for sure it is not “for sure,” to quote Gruber, that such prices are going to fall. (By the way here is an Indiana estimate of rate increases in the range of 70-90%; I can’t vouch for the underlying data. It also seems that price declines are highly likely for New York state, in part because the current system has so many problems. So we also need to be disaggregating the different states here. Also, here is some informal poll evidence for a 30-40% rate increase at the individual level, with some higher increases for some other groups. Caveat emptor, but those would be higher rates and they might even surpass the 3x standard I have set up.)
If you add in President Obama’s varied comments on the matter, I absolutely do see the real truth behind conservative and Republican complaints of “bait and switch.” The median and modal cost of buying non-group health insurance is likely to go up, not down, and not everyone will enjoy the option of keeping the status quo, as had been promised. And that whole matter is being given a different spin today than it was say in 2009. On that Roy is entirely correct.
(In passing, I see employer shedding of coverage as a greater danger to ACA at the macro level, so in my view it is a mistake to see too much of ACA as turning on this issue.)
On the other side of the debate, you will find criticisms of Roy here, here, here, here, and here, among many others. At least two points of the critics seem to stick, first that these may be teaser (status quo) rates sampled by Roy and second we don’t know actually which individuals can end up getting those rates, once they fill out the questionnaires about the earlier medical histories. But even there we are left with “we don’t know” more than “I have better numbers which show Roy to be wrong.” The level of subsidies is relevant too. I think also that Roy’s response undercounts the number of uninsurable people. The worry is not that the market price for insurance is infinite, but rather at the prevailing market price one is simply paying one’s medical bills, plus a processing premium to the insurance company, rather than obtaining ex ante insurance.
To raise two other points critical of Roy’s position, first I am uncomfortable with putting so much emphasis on percentage rate increases, when some of these sums in question may be relatively small. (I find the emphases in Megan’s presentation of the numbers more useful.) I also think it requires a lot more argumentation to measure the number of “those who can’t get useful insurance” than by looking at the number of applications for the high-risk pools, even if that argument ultimately succeeds.
That all said, I find the screeds of most but not all of Roy’s critics to be inappropriate or in some cases beyond inappropriate. It is disturbing how much space and emotional energy is devoted to attacking Roy, and to attacking conservative policy wonkery, relative to trying to calculate the actual extent of rate shock or possible lack thereof. That is not how good policy wonks go about their job.
I think there is quite a good chance we will see rate shock, as I have defined it above. I also think we still don’t know. I also see rhetorical bait and switch from ACA defenders. I also see that Roy is too quick to jump on possible negative information about the California rates without nailing down the case. I also don’t think these are the most important issues for ACA, though they are issues worth discussing.
Overall this is not a debate which is going very well.
Burned by the FDA
 If you lived in Great Britain or Germany and your physician prescribed a pharmaceutical, would you ask them, “has this pharmaceutical been approved by the U.S. FDA?” Probably not. At FDAReview.org Dan Klein and I argue that international reciprocity is a no-brainer:
If you lived in Great Britain or Germany and your physician prescribed a pharmaceutical, would you ask them, “has this pharmaceutical been approved by the U.S. FDA?” Probably not. At FDAReview.org Dan Klein and I argue that international reciprocity is a no-brainer:
If the United States and, say, Great Britain had drug-approval reciprocity, then drugs approved in Britain would gain immediate approval in the United States, and drugs approved in the United States would gain immediate approval in Great Britain. Some countries such as Australia and New Zealand already take into account U.S. approvals when making their own approval decisions. The U.S. government should establish reciprocity with countries that have a proven record of approving safe drugs—including most west European countries, Canada, Japan, and Australia. Such an arrangement would reduce delay and eliminate duplication and wasted resources. By relieving itself of having to review drugs already approved in partner countries, the FDA could review and investigate NDAs more quickly and thoroughly.
Unfortunately, even when they can, the US FDA does not take advantage of international knowledge as the WSJ notes in European Sunscreen Roadblock on U.S. Beaches:
Eight sunscreen ingredient applications have been pending before the U.S. Food and Drug Administration for years—some for up to a decade—for products available in many overseas countries. The applications were filed through the federal TEA process (time and extent application), which allows the FDA to approve the ingredients if they have been used for at least five years abroad and have proved effective and safe.
…Henry Lim, chairman of dermatology at Henry Ford Hospital in Detroit and a member of the American Academy of Dermatology, says multiple UVA filters still awaiting clearance in the U.S. have been used effectively outside the country for years.
“The U.S. is an island by itself on this one,” he said. “They’re available in Canada, available in Europe, available in Asia, available in Mexico, and available in South America.”
The sunscreens available in the U.S. are not without risk and in some ways, as the WSJ discusses, the European standards are stricter than the US standards so there really is no reason why sunscreens available in Europe and Canada should not also be available in the United States.
Hat tip: Kurt Busboom.
Addendum: 27 states have driver’s license reciprocity with Germany. Why not pharmaceutical reciprocity? With hat tip to whatsthat in the comments.