Category: Medicine
Can the Shingles Vaccine Prevent Dementia?
A new paper provides good evidence that the shingles vaccine can prevent dementia, which strongly suggests that some forms of dementia are caused by the varicella zoster virus (VZV), the virus that on initial infection causes chickenpox. The data come from Wales where the herpes zoster vaccine (Zostavax) first became available on September 1 2013 and was rolled out by age. At that time, however, it was decided that the vaccine would only be available to people born on or after September 2 1933. In other words, the vaccine was not made available to 80 year olds but it was made available to 79 year and 364-day olds. (I gather the reasoning was that the benefits of the vaccine decline with age and an arbitrary cut point was chosen.)
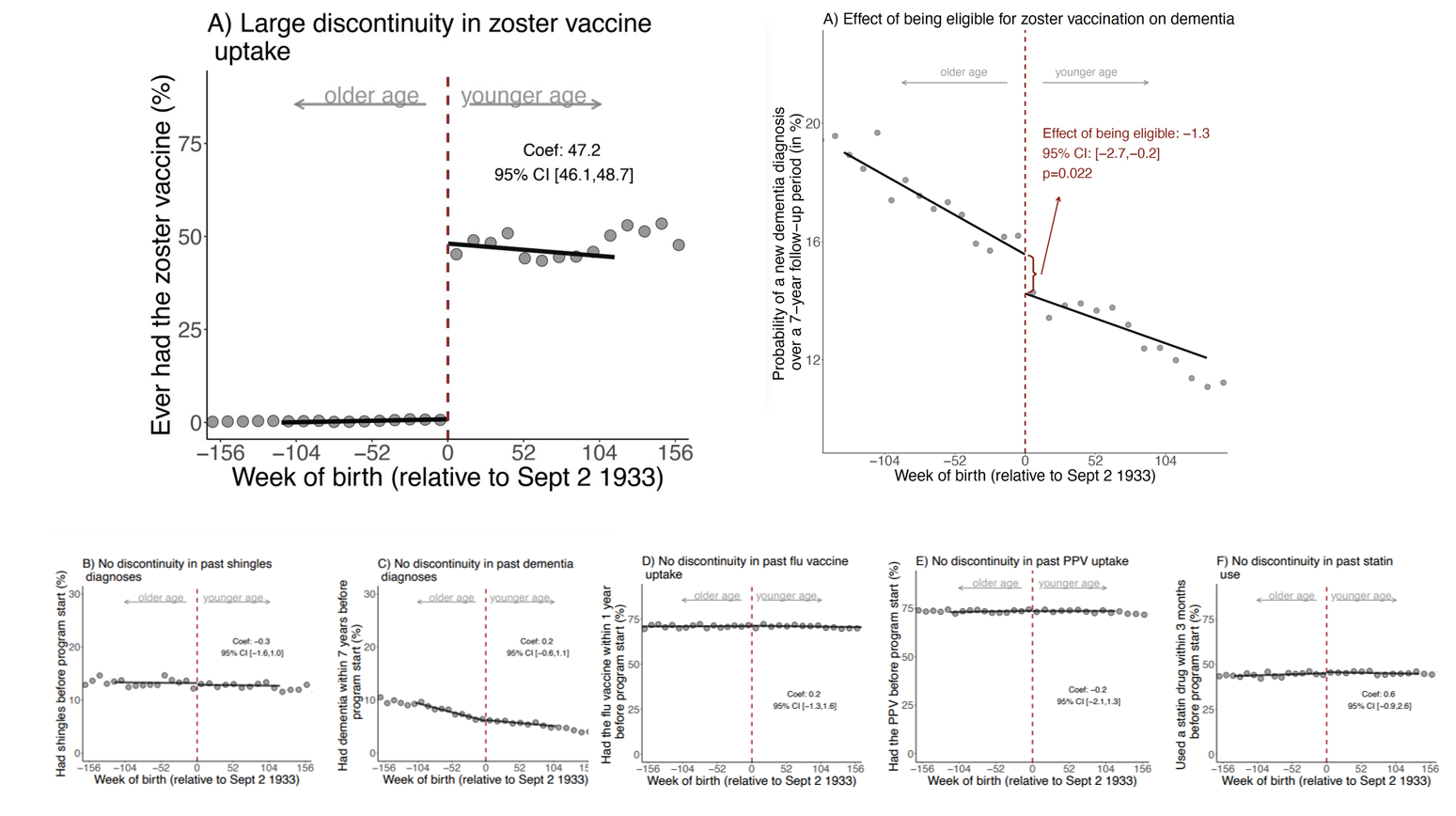
The cutoff date for vaccine eligibility means that people born within a week of one another have very different vaccine uptakes. Indeed, the authors show that only 0.01% of patients who were just one week too old to be eligible were vaccinated compared to 47.2% among those who were just one week younger. The two groups of otherwise similar individuals who were born around September 2 1933 are then tracked for up to seven years, 2013-2020. The individuals who were just “young” enough to be vaccinated are less likely to get shingles compared to the individuals who were slightly too old to be vaccinated (as one would expect if the vaccine is doing it’s job). But, the authors also show that the individuals who were just young enough to be vaccinated are less likely to get dementia compared to the individuals who were slightly too old to be vaccinated, especially among women. A number of robustness tests finds no other sharp discontinuities in treatments or outcomes around the Sept 2, 1933 cut point.
The following graph summarizes. The top left panel shows that the cutoff led to big differences in vaccine uptake, the top right panel shows that there was a smaller but sharp decline in dementia in the vaccinated group. The bottom panel shows that was no discontinuity in a variety of other factors.
Read the whole thing.
I have had my shingles vaccine. As I have said before, vaccination is the gift of a superpower.
The Promising Pathway Act
The evident failures of the FDA and CDC during COVID have opened up new opportunities for reform. One of the most interesting is the Promising Pathway Act, sponsored by Sens. Mike Braun (R-Ind.) and Kirsten Gillibrand (D-N.Y.). As Bart Madden and I write, the Act would create a new form of approval, provisional approval.
The Hill: Here’s how the current version of the bill works: A new drug could secure provisional approval for serious or life-threatening health conditions via early-stage clinical investigations indicating that the new drug’s safety and efficacy compare favorably to approved drugs.
Importantly, provisional approval requires establishing patient registries for all such treatments and is not simply a matter of faster approval. Third-party, independent entities would manage these registries, tracking safety and effectiveness.
In order to speed up the use of this new knowledge, the de-identified, disaggregated databases would be accessible to approved researchers, medical professionals for public health research and biopharmaceutical industry researchers. Drug sponsors or the government would fund the registries, and the FDA would submit an annual report to Congress on provisionally approved drugs.
Thus, provisional approval would allow earlier access to not yet approved drugs but would require the creation of a patient registry and database that could be used by anyone to evaluate the drug. An interesting and important idea.
Ezra Klein and Jean Twenge on teen mental health
They did an NYT podcast, here is the transcript, here is the podcast itself. Excerpt:
EZRA KLEIN: Violent crime actually gets at why I wanted to ask this before we got into smartphones, because I’m much more familiar with the debate over crime than I am over the debate over suicide trend lines. And the thing that has always striking to me, and I think really underplayed in our national discourse over crime, is that we don’t really understand it, that if you go into the ’80s and the ’90s, you see crime goes way, way up in the 70s, way, way up in all kinds of different jurisdictions, more or less all at the same time.
And then it begins going way, way down in all kinds of different places all at the same time. So you have stories that people know, like there’s New York with Rudy Giuliani and broken windows policing and stop and frisk. But it also goes down in all these places that didn’t do what New York City did. It’s so widespread, both the rise and the fall, that you end up having researchers trying to think of even broader explanations, like whether or not lead and the amount of lead in young kids’ bloodstreams — and thus, the effect on their executive function when they got older, maybe that’s the causal mechanism.
And it made me wonder if there isn’t a chance that suicide and teen mental health is like that, that it has this kind of all the way up, all the way down in all places, and we don’t really understand why pattern to it.
Do read/listen to the whole thing, interesting throughout.
Corporate Ownership and Firm Performance: Evidence from Fertility Clinics
Corporate investors are often credited with boosting target firm performance but criticized for prioritizing profits over consumer well-being. This tension is particularly evident in the healthcare sector, where information frictions contribute to underinvestment in quality. This paper finds that corporate ownership can improve healthcare outcomes in a setting where patients have access to service pricing and quality information – the market for In Vitro Fertilization (IVF). After acquisition by a fertility chain, clinic volume increases by 28.2%, and IVF success rates increase by 13.6%. Fertility chains also implement changes that enhance quality, benefit underperforming clinics, and expand the IVF market.
That is from a new paper by Amber La Forgia and Julia Bodner. Via the excellent Kevin Lewis.
The FDA Still Doesn’t Trust Women
The FDA has a long history of antipathy towards personal testing. The FDA has opposed personal pregnancy tests, HIV tests, genetic tests, and COVID tests, as I discussed in my article Testing Freedom. Well, the FDA is at it again:
NYTimes: At a hearing Tuesday to consider whether the Food and Drug Administration should authorize the country’s first over-the-counter birth control pill, a panel of independent medical experts advising the agency was left to reckon with two contradictory analyses of the medication called Opill.
During the eight-hour session, the manufacturer of the pill, HRA Pharma, which is owned by Perrigo, and representatives of many medical organizations and reproductive health specialists said that data strongly supported approval. They said that Opill, approved as a prescription drug 50 years ago, was safe, effective and easy for women of all ages to use appropriately — and that over-the-counter availability was sorely needed to lower the country’s high rate of unintended pregnancies.
In contrast, F.D.A. scientists questioned the reliability of company data that was intended to show that consumers would take the pill at roughly the same time every day and comply with directions to abstain from sex or temporarily use other birth control if they missed a dose. The agency seemed especially concerned about whether women with breast cancer or unexplained vaginal bleeding would correctly choose not to take Opill and whether adolescents and people with limited literacy would use it accurately.
Note carefully: The FDA isn’t worried that women won’t take the pill at the same time every day they are worried that women who get the pill without a prescription won’t take it at the same time every day. I guess in the FDA’s view women need some mansplaining to take birth control or at least some doctorplaining.
Dr. Westhoff suggested that for most women, there is no advantage to a doctor prescribing the pills because doctors don’t typically monitor patient adherence and often only see such patients once a year.
Similarly, I suspect that women with breast cancer will be concerned enough about their health to read the warning, Don’t Take This Pill if You Have Breast Cancer. Who knows, women with breast cancer might even ask their cancer physician or Google or their GP(T) about what foods and drugs to take and which to avoid.
If I didn’t know the FDA’s long history of opposing personal testing, I would think this simply bizarre but not trusting people with their own health decisions is practically in the FDA’s DNA.
Polish Vending Machine for Contact Lenses

Here’s one in Lithuania. See my post The Optometry Racket for more on the context.
Hat tip: Tadeusz Giczan.
From the Comments
The context is that human challenge trials were “ethically fraught” but, Sure writes:
…I think we had more than a few instances in history where restricting movement, shuttering houses of worship, and stratifying the economy into favored and disfavored sectors was considered ethically fraught.
I mean we know that limiting visitation to old folks shortens their lives. We know that child abuse becomes harder to find the fewer the number of folks who lay eyes on them each day. We know that initimate partner violence increases when the housing market gets frozen. And we know that suicides crest when businesses go under.
Yet no such epistemic humility and wariness followed with public health recommendations to be tried on a scale reserved hitherto for literal wars and genocides. And we blindly went ahead full speed.
Or consider even the better defined but wildly more mundane issue: proof of vaccination. For decades health ethicists told us that merely revealing a patient’s name, let alone which medications they have taken, was an unconscionable ethical violation. One which we instituted balkanized medical systems to manage and where the cost has been literal lives lost as we have had untold numbers of patients fall through the cracks thanks to duplicate profiles, failure of providers to communicate, and of course scads and scads of useful data locked away from effective statistical analysis that could spot patterns of medical error.
Yet when the powers that be decided that we needed vaccine passports so we could enjoy dining again? Well, every waiter in the country becomes a safe repository of PHI.
No formal study. No deliberations. Precious little if any publications.
And even then, it went only for what was the most expedient option for the enlightened. No ability to get an antibody titer card for medical equivalence. No ability to substitute PCR results with a physician evaluation of recent disease recovery.
Professional medical ethics are bogus. There is no consistency and the entire profession serves to pander to the prejudices of the educated.
A Systematic Review of Human Challenge Trials, Designs, and Safety
One of the most bizarre aspects of the COVID era was the institutional unwillingness to perform human challenge trials, which likely would have sped up vaccines and other treatments and saved lives. We let people join the military, indeed we advertise to encourage people to join the military, but for some reason running a human challenge trial is considered ethically fraught.
A new review find that HCTs are quite safe–more evidence that we have too few of these trials.
Human challenge trials (HCTs) are a clinical research method in which volunteers are exposed to a pathogen to derive scientifically useful information about the pathogen and/or an intervention [1]. Such trials have been conducted with ethical oversight since the development of the modern institutional review system of clinical trials in the 1970s. More recently, there has been renewed discussion about the ethical and practical aspects of conducting HCTs, largely fueled by interest in conducting HCTs for severe acute respiratory syndrome coronavirus 2. Past reviews of HCTs focused on reporting methods [2] and safety for single pathogens [3–6], but these did not explicitly evaluate the safety of HCTs by assessing reported adverse events (AEs) and serious adverse events (SAEs) across a range of pathogens. Furthermore, many additional HCTs have been performed since the publication of these reviews. To better inform discussions about future uses of HCTs, including during pandemic response, this article presents a systematic review of challenge trials since 1980 and reports on their clinical outcomes, with particular focus on risk of AEs and risk mitigation strategies.
Hat tip: Alec Stapp.
*The AI Revolution in Medicine: GPT-4 and Beyond*
A new, forthcoming book by Peter Lee, Carey Goldberg, and Isaac Kohane, with Sebastian Bubeck. The researchers were given advance access to GPT-4 (with no editorial controls), and this book documents the power of the results, for instance:
In our testing, when given a full battery of USMLE [medical licensing exam] problems, GPT-4 answers them correctly more than 90 percent of the time.
And it can give very good explanations.
Due out May 13, this book is the documentation, definitely recommended, especially for the skeptics.
The polity that is Russian markets in everything
In Russian prisons, they said they were deprived of effective treatments for their H.I.V. On the battlefield in Ukraine, they were offered hope, with the promise of anti-viral medications if they agreed to fight.
It was a recruiting pitch that worked for many Russian prisoners.
About 20 percent of recruits in Russian prisoner units are H.I.V. positive, Ukrainian authorities estimate based on infection rates in captured soldiers. Serving on the front lines seemed less risky than staying in prison, the detainees said in interviews with The New York Times.
Here is the full NYT story. And here is how it unfolded:
Timur had no military experience and was provided two weeks of training before deployment to the front, he said. He was issued a Kalashnikov rifle, 120 bullets, an armored vest and a helmet for the assault. Before sending the soldiers forward, he said, commanders “repeated many times, ‘if you try to leave this field, we will shoot you.’”
Soldiers in his platoon, he said, were sent on a risky assault, waves of soldiers with little chance of survival sent into battle on the outskirts of the eastern city of Bakhmut. Most were killed on their first day of combat. Timur was captured.
Roughly ten percent of Russia’s incarcerated population has signed up to fight in Ukraine.
Measuring the benefits of the biomedical revolution
That is the topic of my latest Bloomberg column. Note that for most economic gains, total gdp and per capita gdp give roughly the same answers. But when it comes to lifesaving, that may no longer be the case. Here is one excerpt:
Take the vaccines against Covid. Of course the most important fact about them is that they reduce the amount of death and suffering. But what is their economic impact? The vaccines have been most helpful to the most vulnerable, namely the elderly or those with preexisting medical conditions. These are not the most productive cohorts of the economy. So the effectiveness of the vaccines might have actually lowered various social averages, such as per-capita GDP or per-capita productivity.
The extra life is a pure benefit. But to capture that benefit in numbers requires looking at the totals, not just the averages. Labor productivity per hour, for example, won’t necessarily increase. But total labor supply and total population will.
And this:
And what about those subpar returns on biomedical investments? That is a sign that most of the gains from innovation are being reaped by patients, users and consumers — not capitalists. Is that not exactly what everyone has been asking for?
There is much more at the link. The bottom line is that many of the gains will come through “n,” not per hour productivity.
A new Operation Warp Speed for better vaccines
The Biden administration is launching a $5 billion-plus program to accelerate development of new coronavirus vaccines and treatments, seeking to better protect against a still-mutating virus, as well as other coronaviruses that might threaten us in the future.
“Project Next Gen” — the long-anticipated follow-up to “Operation Warp Speed,” the Trump-era program that sped coronavirus vaccines to patients in 2020 — would take a similar approach to partnering with private-sector companies to expedite development of vaccines and therapies. Scientists, public heath experts and politicians have called for the initiative, warning that existing therapies have steadily lost their effectiveness and that new ones are needed…
Jha and others said the new effort will focus on three goals: creating long-lasting monoclonal antibodies, after an evolving virus rendered many current treatments ineffective; accelerating development of vaccines that produce mucosal immunity, which is thought to reduce transmission and infection risks; and speeding efforts to develop pan-coronavirus vaccines to guard against new SARS-CoV-2 variants, as well as other coronaviruses.
Here is the WaPo article, here is commentary from Eric Topol.
The case for nurse practitioners
Many states have recently changed their scope of practice laws and granted full practice authority to nurse practitioners, allowing them to practice without oversight from physicians. Physician groups have argued against this change, citing patient safety concerns. In this paper, we use a ratio-in-ratio approach to evaluate whether the transition to full practice authority results in harm to patients as proxied by rates of malpractice payouts and adverse action reports against nurse practitioners. We find no evidence of such harm, and instead find that physicians may benefit from the law change in terms of reduced malpractice payouts against them.
That is from a new NBER working paper by Sara Markowitz and Andrew J.D. Smith.
Peltzman Revisited
Casey Mulligan has an excellent new paper, Peltzman Revisited: Quantifying 21st-Century Opportunity Costs of Food and Drug Administration Regulation. What are the costs of delaying a new drug or a vaccine? Longer and bigger clinical trials increase safety but I’ve often made the point that the people who would have lived had a good drug been approved sooner are buried in an invisible graveyard and thus these costs are typically undercounted–the failure to see the invisible graveyard biases decisions in favor of delay. Mulligan makes a different and rarely considered point about substitution effects. If a vaccine isn’t available there are substitutes but these substitutes are themselves potentially unsafe and ineffective. But who is testing the substitures?
Many of these substitute interventions, such as remote work, closing schools, and canceling normal medical appointments, are beyond the jurisdiction of the FDA and can be utilized without any attempt to demonstrate their safety or efficacy.
If the substitutes work, the costs of delay are reduced. The FDA, for example, is right to prioritize drugs for which there are few alternative treatments. But the standards for many vaccine or drug substitutes are completely different than those used to approve a vaccine:
Closing schools to in-person learning is an important example of a prevention activity that was available, was applied to tens of millions of children in the United States, and was outside the FDA’s jurisdiction…Obviously the FDA’s effectiveness standard for vaccines differs from the effectiveness standard (if any) that school districts applied in deciding to close schools.
Where were the randomized controlled trials for closing schools, shutting the parks and beaches, and delaying medical appointments? Thus, it’s quite possible that greater safety of vaccines comes at the expense of greater time under less safe and possibly unsafe substitutes. As Mulligan concludes:
Approval delays for pandemic tests and vaccines pushed tens of millions of individuals and businesses into preventions and treatments that were both outside FDA jurisdiction and hardly safe or effective. The pandemic experience raises the question of whether, on the whole, consumers engage in more unsafe and ineffective practices than they would if FDA approval were not a prerequisite for pharmaceutical sales.
Addendum: Much else of interest in the paper including a calculation of the value of the vaccines in the hundreds of billions and trillions very much in line with work done by the AHT team, including myself ,in the AER PP (especially the appendix) and Science.
GPT-4 Does the Medical Rounds
GPT4 passed the medical licensure exam but the critics want to know how does it perform in the real world? Zak Kohane, pediatric endocrinologist, data scientist, and chair of the Harvard Chair of the Department of Biomedical Informatics at Harvard Medical School has apparently been working with GPT4 for about 6 months. He has a forthcoming book (with Peter Lee and Carey Goldberg). He writes:
“How well does the AI perform clinically? And my answer is, I’m stunned to say: Better than many doctors I’ve observed.”—Isaac Kohane MD
That’s from a review of the book by Eric Topol. Not much more information to be had in the review but if you think about it, this bit is hilarious:
I’ve thought it would be pretty darn difficult to see machines express empathy, but there are many interactions that suggest this is not only achievable but can even be used to coach clinicians to be more sensitive and empathic with their communication to patients.