Category: Medicine
Ross Douthat on the burden and incidence of ACA
As Angus has pointed out, Ross has been on a real roll lately, here is yet another good bit:
Now an effective levy of several thousand dollars on the small fraction of middle class Americans who buy on the individual market is not history’s great injustice. But neither does it seem like the soundest or most politically stable public policy arrangement. And to dig back into the position where I do strong disagree with Cohn’s perspective, what makes this setup potentially more perverse is that it raises rates most sharply on precisely those Americans who up until now were doing roughly what we should want more health insurance purchasers to do: Economizing, comparison shopping, avoiding paying for coverage they don’t need, and buying a level of insurance that covers them in the event of a true disaster while giving them a reason not to overspend on everyday health expenses.
If we want health inflation to stay low and health care costs to be less of an anchor on advancement, we should want more Americans making $50,000 or $60,000 or $70,000 to spend less upfront on health insurance, rather than using regulatory pressure to induce them to spend more. And seen in that light, the potential problem with Obamacare’s regulation-driven “rate shock” isn’t that it doesn’t let everyone keep their pre-existing plans. It’s that it cancels plans, and raises rates, for people who were doing their part to keep all of our costs low.
The full post is here.
What is the most likely path forward for the ACA exchanges?
I had lunch yesterday with a friend and I was asked that question (and I asked it in turn). My answer, with some ex post editing, was this:
1. The chance of “no smooth resolution” for the health care exchanges crisis is now 60-40. Not long ago I thought it was 20-80.
2. The Obama administration is claiming the exchanges might be ready soon to stem Democratic defections and to keep the policy locked in, but in reality they now know there is no chance for timeliness (NB: this sentence is true with 60-40 probability, not unconditionally true).
3. More parts of the thing will be working by late November, but not enough for it to serve as a functioning enrollment system, much less encourage “the invincibles” to sign up. They will figure, correctly, they don’t have to bother with the whole thing until they hear from peers, and from the media, that the process is as smooth and as easy as Orbitz. (Oddly, Tea Party attempts to get young people to resist the mandate have the counterintuitive property of increasing awareness of the sign up requirement. Disengagement, not fiery opposition, is the real enemy of the law.)
4. Come January 1, hundreds of thousands of Americans will lose their individual coverage packages for not meeting ACA standards. Most of them won’t have ready replacements. This will be a big mainstream media story, not just a FoxNews story. There will be easily identifiable victims, expressing sorrow or rage or both in front of the camera. Left-wing bloggers will express outrage that Republicans express outrage over the existence of individuals with no insurance coverage. Republicans will express outrage that left-wing bloggers express outrage, etc.
5. Democrats will propose various ACA fixes, and Republicans will reject them, claiming that the law requires a more fundamental restructuring. That standoff will not be readily resolved and it will become the “new debt-ceiling crisis.” Democratic defections will be a problem for Obama.
6. The exchanges will be mostly working by March 2014, but by then the risk pool will be dysfunctional. In the meantime, real net prices will creep up, if only through implicit rationing and restrictions on provider networks. The Obama administration will attempt to address this problem — unsuccessfully — through additional regulation.
7. By October 2014, no one will think the exchanges are a satisfactory solution, except for 17 state exchanges which will be running reasonably well. Some of the state-level exchanges, by the way, will have more serious problems than is currently evident, mostly on the back end.
8. Chris Christie will campaign against ACA and beat Hillary Clinton in the general election. Upon assuming office he will place price controls on the insurance plans in the individual market, repeal much but not all of the federal financial support for the Medicaid expansion, and keep many other parts of ACA, while claiming to have repealed the whole thing. Enough Democrats will go along with this, as public opinion will have shifted toward the Republican side on this issue. The individual market still won’t be working very well. The exchanges will be working fine in the technical sense, but skittishness, political risk, and the adverse selection death spiral will have led the insurance companies to withhold high quality policies from that side of the market.
From the comments (Dan Hanson on ACA)
Dan writes:
The front end technology is not the problem here. It would be nice if it was the problem, because web page scaling issues are known problems and relatively easy to solve.
The real problems are with the back end of the software. When you try to get a quote for health insurance, the system has to connect to computers at the IRS, the VA, Medicaid/CHIP, various state agencies, Treasury, and HHS. They also have to connect to all the health plan carriers to get pre-subsidy pricing. All of these queries receive data that is then fed into the online calculator to give you a price. If any of these queries fails, the whole transaction fails.
Most of these systems are old legacy systems with their own unique data formats. Some have been around since the 1960′s, and the people who wrote the code that runs on them are long gone. If one of these old crappy systems takes too long to respond, the transaction times out.
Amazingly, none of this was tested until a week or two before the rollout, and the tests failed. They released the web site to the public anyway – an act which would border on criminal negligence if it was done in the private sector and someone was harmed. Their load tests crashed the system with only 200 simultaneous transactions – a load that even the worst-written front-end software could easily handle.
When you even contemplate bringing an old legacy system into a large-scale web project, you should do load testing on that system as part of the feasibility process before you ever write a line of production code, because if those old servers can’t handle the load, your whole project is dead in the water if you are forced to rely on them. There are no easy fixes for the fact that a 30 year old mainframe can not handle thousands of simultaneous queries. And upgrading all the back-end systems is a bigger job than the web site itself. Some of those systems are still there because attempts to upgrade them failed in the past. Too much legacy software, too many other co-reliant systems, etc. So if they aren’t going to handle the job, you need a completely different design for your public portal.
A lot of focus has been on the front-end code, because that’s the code that we can inspect, and it’s the code that lots of amateur web programmers are familiar with, so everyone’s got an opinion. And sure, it’s horribly written in many places. But in systems like this the problems that keep you up at night are almost always in the back-end integration.
The root problem was horrific management. The end result is a system built incorrectly and shipped without doing the kind of testing that sound engineering practices call for. These aren’t ‘mistakes’, they are the result of gross negligence, ignorance, and the violation of engineering best practices at just about every step of the way..
…“No way would Apple, Amazon, UPS, FedEx outsource their computer systems and software development, or their IT operations, to anyone else.”
You have to be kidding. How do you think SAP makes a living? Or Oracle? Or PeopleSoft? Or IBM, which has become little more than an IT service provider to other companies?
Everyone outsources large portions of their IT, and they should. It’s called specialization and division of labor. If FedEx’s core competence is not in IT, they should outsource their IT to people who know what they are doing.
In fact, the failure of Obamacare’s web portal can be more reasonably blamed on the government’s unwillingness to outsource the key piece of the project – the integration lead. Rather than hiring an outside integration lead and giving them responsibility for delivering on time, for some inexplicable reason the administration decided to make the Center for Medicare and Medicaid services the integration lead for a massive IT project despite the fact that CMS has no experience managing large IT projects.
Failure isn’t rare for government IT projects – it’s the norm. Over 90% of them fail to deliver on time and on budget. But more frighteningly, over 40% of them fail absolutely and are never delivered. This is because the core requirements for a successful project – solid up-front analysis and requirements, tight control over requirements changes, and clear coordination of responsibility with accountability, are all things that government tends to be very poor at,
The mystery is why we keep letting them try.
Arnold Kling on the problems with the health insurance exchanges
Somebody who had experience with creating a health insurance brokerage business would know that the systems problems are more complicated than just putting up a web site. In the background, the system needs to communicate with the systems at several government agencies and at the insurance companies. That changes it from a simple technical project to a complex, time-consuming, project involving business and technical staff.
You build a complex, mission-critical system through a process of continual negotiations among business units and technical people. You do not treat it as a procurement process. You cannot just write up a spec, put it up for bid, and parcel it out to dozens of contractors.
The development of the computer system probably would fall under operations, but you would want a project executive with a lot of authority to negotiate with all of the business units and to make project decisions. When conflicts arise, the project executive should be able to go straight to the CEO and get them resolved.
The project executive’s main focus is keeping the project’s complexity from getting out of control. The project executive must have the authority to trim features in order to meet deadlines.
You go through a lot of analysis and many painful meetings before anyone writes a line of code. The technical staff have to be able to challenge the business units, because sometimes the business unit asks for something to be done in a really complicated way, when a much simpler solution is available to solve the business problem.
One of the worst things that can happen on a systems project is to find yourself revisiting the business-technical negotiations process after writing a lot of code. If that is what is happening now, this project is in an unbelievable amount of trouble.
5. I suspect that the technical problems are mere symptoms. Probably what is fundamentally messed up in this health insurance brokerage business is the org chart.
There is more here.
Saving Lives with Distributed Intelligence
One of the general features of information technology is that through coordination it makes better use of distributed resources, such as workers, automobiles or energy. An excellent case in point is being tested in Stockholm, Sweden. SMSlivräddare (in Swedish) has a large list of people who are trained in cardiopulmonary resuscitation (CPR). When an emergency call is received indicating a possible heart attack, SMSlivräddare finds the mobile phone user(s) closest to the potential victim and alerts them with a text message. The message also contains a map to the victim’s location.
Survival rates for heart attack outside a hospital in Sweden are low, only about 5-10% but every minute shaved off the time it takes to begin CPR increases the survival rate by 10%. When notified, SMS responders arrive faster than ambulances about 50% of the time so the potential for saving lives is quite large (final data on the research project are not yet in).
Could such a system work in the United States? Maybe, a similar but more passive app is available in a few locations. Legal issues are a threat. Good Samaritan laws offer some protection although they often apply only to medical professionals. The threat, however, is not really to the responder but to the service. It’s interesting to watch Shark Tank, anytime a medical entrepreneur makes an appearance the sharks run away for fear of liability. Still, if the service were attached to a hospital and integrated with ambulances services, it ought to be possible to be insulated but this will require significant political entrepreneurship.
Hat tip: Connor Tabarrok.
Bubonic Plague
BBC: Madagascar faces a bubonic plague epidemic unless it slows the spread of the disease, experts have warned. The Red Cross and Pasteur Institute say inmates in the island’s rat-infested jails are particularly at risk.
…Madagascar had 256 plague cases and 60 deaths last year, the world’s highest recorded number.
Bubonic plague, known as the Black Death when it killed an estimated 25 million people in Europe during the Middle Ages, is now rare.
“If the plague gets into prisons there could be a sort of atomic explosion of plague within the town. The prison walls will never prevent the plague from getting out and invading the rest of the town,” said the institute’s Christophe Rogier.
Have a nice day.
How to reform Obamacare
Obviously we remain in a gridlocked political period, but if a new deal on health care reform could be cut, what would it look like? What should it look like? In my latest New York Times column I attempt to peer into that future. Here is one excerpt:
One way forward would look like this: Federalize Medicaid, remove its obligations from state budgets altogether and gradually shift people from Medicaid into the health care exchanges and the network of federal insurance subsidies. One benefit would be that private insurance coverage brings better care access than Medicaid, which many doctors are reluctant to accept.
To help pay for such a major shift, the federal government would cut back on revenue sharing with the states and repeal the deductibility of state income taxes. The states should be able to afford these changes because a big financial obligation would be removed from their budgets.
By moving people from Medicaid to Obamacare, the Democrats could claim a major coverage expansion, an improvement in the quality of care and access for the poor, and a stabilization of President Obama’s legacy — even if the result isn’t exactly the Affordable Care Act as it was enacted. The Republicans could claim that they did away with Medicaid, expanded the private insurance market, and moved the nation closer to a flat-tax system by eliminating some deductions, namely those for state income taxes paid.
At the same time, I’d recommend narrowing the scope of required insurance to focus on catastrophic expenses. If insurance picks up too many small expenses, it encourages abuse and overuse of scarce resources.
The full column is here. Please allow me to add a few remarks which did not fit into the column proper (which is strictly limited at 900 words):
1. My argument does presuppose that the exchanges can at the technical level, in some manner, end up working for enough states to carry this option forward. I still think this is likely, but today it appears less likely than even a week ago when I drafted the column. The biggest danger is that we enter an “adverse selection death spiral,” even if the technical problems eventually get fixed. It has to be seen as easy for young, healthy people to buy health insurance on the exchanges, otherwise they probably will not work.
2. I view this reform as more likely to come through a Republican President than a Democrat. A Republican has to do something which counts as “getting rid of Obamacare,” yet simply returning to the status quo ex ante would not be so popular with mainstream voters. This is the most likely direction for such reforms.
3. I did not have enough space to talk about more immigration for physicians and nurses, liability reform, and other supply-side reforms. They are very important.
4. I have been reading for years that ACA is just like the health care reform proposal from The Heritage Foundation from the early 1990s. Well, sort of. I view the proposal in my column as closer to the ideas many conservatives were pushing in the 1990s. But if they are indeed “the same thing,” then fine, there should be no problem supporting one rather than the other!
5. I view my proposal as a third- or fourth-best exercise, it is neither first nor second best. It may be the best we can do from where we stand, subject to the caveats in #1 however.
Here are some related remarks from Ross Douthat. He argues that conservatives should be hoping that the exchanges succeed, because the relevant alternatives are worse and because the exchanges themselves can serve as a foundation for future reforms.
How Medicare influences private payment systems (model this)
There is a new paper by Jeffrey Clemens and Joshua D. Gottlieb on this topic, the abstract is here:
We analyze Medicare’s influence on private payments for physicians’ services. Using a large administrative change in payments for surgical procedures relative to other medical services, we find that private payments follow Medicare’s lead. On average, a $1 change in Medicare’s relative payments results in a $1.30 change in private payments. We find that Medicare similarly moves the level of private payments when it alters fees across the board. Medicare thus strongly influences both relative valuations and aggregate expenditures on physicians’ services. We show further that Medicare’s price transmission is strongest in markets with large numbers of physicians and low provider consolidation. Transaction and bargaining costs may lead the development of payment systems to suffer from a classic coordination problem. By extension, improvements in Medicare’s payment models may have the qualities of public goods.
This paper, which seems quite sound to me, has a few implications.
First, if you are unhappy with the American health care system, government is more at fault for the problems of the private sector than it may at first appear. We have a much more governmental system than most of its critics care to admit and that goes even beyond government health care spending as a percentage of total health care spending.
Second, we could cut Medicare reimbursement rates, by limiting the doc fix, without old people all very rapidly going to the back of the health care queue.
Third, the authors find that the larger Medicare becomes, the stronger this “pass through” effect generally will be. In other words, this result will be all the more true in our future.
Fourth, the cross-sectoral price transmission result implies that long-run supply elasticities in the sector are not large, which also does not bode well for the future of health care access in an aging society.
Overall this is a depressing paper, although it implies that successful Medicare cost control could have significant cross-sectoral benefits, beyond Medicare itself.
The Quality Of Care Delivered To Patients Within The Same Hospital Varies By Insurance Type
That is the new paper by Christine S. Spencer, Darrell J. Gaskin, and Eric T. Roberts. Let me excerpt the three most important sentences from the abstract:
We found that privately insured patients had lower risk-adjusted mortality rates than did Medicare enrollees for twelve out of fifteen quality measures examined. To a lesser extent, privately insured patients also had lower risk-adjusted mortality rates than those in other payer groups. Medicare patients appeared particularly vulnerable to receiving inferior care.
I don’t have a great deal of confidence in our ability to estimate the size of that effect, but keep that difference in mind next time someone tells you that Medicare is so much more efficient than private health insurance in this country.
Equilibria in health exchanges
There is a recent paper (pdf) by Handel, Hendel, and Whinston, and it covers the issue of adverse selection through the new ACA exchanges. The second paragraph of the abstract is this:
We find that market unravelling from adverse selection is substantial under the proposed pricing rules in the Affordable Care Act (ACA), implying limited coverage for individuals beyond the lowest coverage (Bronze) health plan permitted. Although adverse selection can be attenuated by allowing (partial) pricing of health status, our estimated risk preferences imply that this would create a welfare loss from reclassification risk that is substantially larger than the gains from increasing within-year coverage, provided that consumers can borrow when young to smooth consumption or that age-based pricing is allowed. We extend the analysis to investigate some related issues, including (i) age-based pricing regulation (ii) exchange participation if the individual mandate is unenforceable and (iii) insurer risk-adjustment transfers.
The core result here does not require individuals to violate the legal mandate, although the paper has a good and sobering discussion of that topic as well. The adverse selection here is occurring across plans of differing quality. On the positive side, having everyone enrolled in the “least comprehensive” plan can be a plus rather than a minus, depending on your point of view. On the negative side, the paper does not consider how suppliers might respond by limiting the quality of their network and making the least comprehensive plan even less useful.
For the pointer I thank Dan in Euroland.
Bob Laszlewski on the ACA exchanges
Based upon my survey of a large number of health plans accounting for substantial market share in the 36 states the federal insurance exchange is operating in, not more than about 5,000 individuals and families signed-up for health insurance in the 36 states run by the Obama administration through Monday.
It is not uncommon for a major health insurer with a large market share to report less than 100 enrollments in the first week.
Reports today say the enrollments continue to trickle in at about the same rate.
Worse, the backroom connection between the insurance companies and the federal government is a disaster. Things are worse behind the curtain than in front of it.
Here is one example from a carrier–and I have received numerous reports from many other carriers with exactly the same problem. One carrier exec told me that yesterday they got 7 transactions for 1 person – 4 enrollments and 3 cancellations.
For some reason the system is enrolling, unenrolling, enrolling again, and so forth the same person. This has been going on for a few days for many of the enrollments being sent to the health plans. It has got on to the point that the health plans worry some of these very few enrollments really don’t exist.
The reconciliation system, that reconciles enrollment between the feds and the health plans, is not working and hasn’t even been tested yet.
When health plans call the special health plan “help desk” they are lucky to get through. When they finally get through, the feds are creating a “help desk ticket” to be researched.
Now, if we are enrolling 20 to 50 people per day per health plan per state through the federal exchange, that might be sort of manageable. But if this thing ever ramps up to thousands of enrollments a day…
In summary, big market share health plans are getting maybe 50 enrollments per day per state from the feds and that little bit of new business is a mess.
The link is here, hat tip goes to virtually everyone in my Twitter feed.
Will the health care exchanges lower prices over time?
Here are some interesting arguments from David Goldhill, here is one of them:
The designers of the health-care exchanges have also assumed that consumers, by shopping for the best deal, will drive down premiums. However, a major flaw in the design of insurance subsidies will insulate almost all of the initial customers — the estimated 20 million subsidized households — from concern about how much their policies cost.
Now, it’s not supposed to work this way. Only those Americans who don’t get insurance at work and who have income that puts them between 100 percent (138 percent in Medicaid expansion states) and 400 percent of the federal poverty level are eligible for exchange subsidies. As income rises within this bracket, the subsidy shrinks. But in practical terms, everyone who is subsidized has an infinite subsidy that will make them insensitive to premium levels.
How can that be? Let’s take an example. A family of four at 138 percent of the poverty level ($32,499) has its premium capped at 3.29 percent of income or $1,071. The rest is subsidy. So, if the cost of a silver plan is $10,000, the subsidy for this family is $8,929. A family at 400 percent of the poverty level ($94,200) has to pay up to 9.5 percent of its income for a plan, or $8,949. So the same $10,000 premium carries a subsidy of only $1,051.
…But now look at those two families from the insurer’s perspective. A $10,000 plan already costs more than the maximum amount either family would pay. If the insurer raises the premium to $10,001, both families get $1 in additional subsidy. If it raises premiums to $11,000, both families get $1,000 in additional subsidy. In other words, no matter how much an insurer raises rates, a subsidized household pays zero more.
The full piece is here. Reihan adds useful comments. This evidence does indicate that more sellers does lead to lower premiums, relative to fewer sellers.
The back end glitches in Obamacare
Very few of the individuals trying to buy health insurance are getting through to all the steps of the federal ACA website and using it successfully. But once they register, they still may not have actual coverage plans, with successes running at what is (possibly) a one in one hundred rate:
As few as 1 in 100 applications on the federal exchange contains enough information to enroll the applicant in a plan, several insurance industry sources told CNBC on Friday. Some of the problems involve how the exchange’s software collects and verifies an applicant’s data.
“It is extraordinary that these systems weren’t ready,” said Sumit Nijhawan, CEO of Infogix, which handles data integrity issues for major insurers including WellPoint and Cigna, as well as multiple Blue Cross Blue Shield affiliates.
Experts said that if Healthcare.gov‘s success rate doesn’t improve within the next month or so, federal officials could face a situation in January in which relatively large numbers of people believe they have coverage starting that month, but whose enrollment applications are have not been processed.
There is more here, via Megan McArdle, who for years has been predicting major problems with the web sites. By the way, these are not fundamentally problems of high usage or high demand.
Average is Over
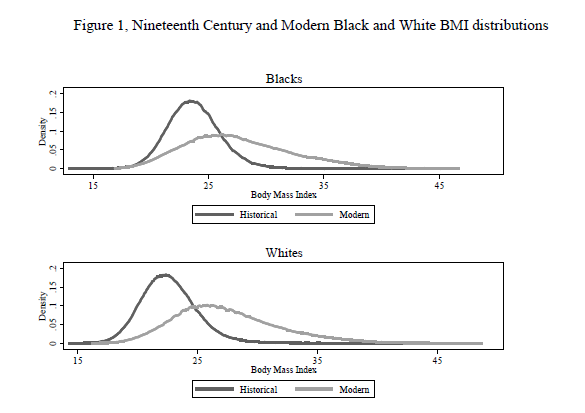
There has been an increase in the mean body-mass index since the 19th century but even more strikingly there has been an increase in the variance, what we might call an increase in weight inequality. More here.
Hat tip: Andrew Leigh.
Further small steps toward designer babies
A personal-genomics company in California has been awarded a broad U.S. patent for a technique that could be used in a fertility clinic to create babies with selected traits, as the frontiers of genetic enhancement continue to advance.
The patented process from 23andMe, whose main business is collecting DNA from customers and analyzing it to provide information about health and ancestry, could be employed to match the genetic profile of a would-be parent to that of donor sperm or eggs. In theory, this could lead to the advent of “designer babies,” a controversial idea where genes would be selected to boost the chances of a child having certain physical attributes, such as a particular eye or hair color.
The technique potentially could also be used to create healthier babies, by screening out donors with genes that are predisposed to disease, either on their own, or in combination with the recipient’s genes.
The awarding of the patent “is a massive addition to what is currently being done” in fertility clinics, said Sigrid Sterckx of the Bioethics Institute Ghent in Belgium, who co-wrote a commentary on the 23andMe patent in the journal Genetics in Medicine on Thursday. “It indicates a different attitude, not just about disease-related traits, but nondisease traits.” 23andMe, based in Mountain View, Calif., says that while its new patent encompasses trait selection in babies, through a tool called the Family Traits Inheritance Calculator, it has no plans to apply it to that end.
As I understand the article, this works only when there is a sperm or egg donor, although a potential marrying couple could use it ex ante (“come on Biff, let’s just try it, I’m just curious. I’ll always love you.”) My view has long been that most people, if they have the chance, are willing to embrace and also use eugenics, albeit with some reframing and rebranding. Eugenics was a very popular idea with Progressives earlier in the twentieth century, and also with economists (in particular, pdf), and ultimately the Nazi connection will be seen as a bump in the road. Competition with the Chinese will help push Americans toward this ideological shift. I am more skeptical myself, as I see greater value in the genetic outliers and I fear their disappearance or diminution. I also am relatively skeptical about the quality of the processes — legal and otherwise — which are likely to govern such experiments. In any case, you can think of this as the next step after “early intervention.” Why don’t we call it “very early intervention”?
The story is here, and if you need to get through the gate, enter “Gautam Naik”, the author of the article, into news.google.com.