Category: Medicine
The new Obama plan to combat antibiotic overuse
The Obama administration on Thursday announced measures to tackle the growing threat of antibiotic resistance, outlining a national strategy that includes incentives to spur the development of new drugs, tighter stewardship of existing ones and a national tracking system for antibiotic-resistant illness. The actions are part of the first major federal effort to confront a public health crisis that takes at least 23,000 lives a year.
The full story is here.
The Hill has more detail. It is an executive order:
The president’s directive creates the Task Force for Combating Antibiotic-Resistant Bacteria, co-chaired by the secretaries of Defense, Agriculture and Health and Human Services.
The group is charged with implementing a plan to track and prevent the spread of antibiotic-resistant bacteria, promote better practices for the use of current drugs and push for a new generation of antibiotic medications.
To that end, the White House on Thursday announced a $20 million prize “to facilitate the development of rapid, point-of-care diagnostic tests for healthcare providers to identify highly resistant bacterial infections.”
The added incentive and the timeframe given to the task force indicate the urgency with which the administration is acting, said Dr. Eric Lander, who co-chairs the President’s Council of Advisors on Science and Technology.
“This is a pretty tight timeline to now come up with a national game plan,” Lander said.
There is also this:
In December, the Food and Drug Administration (FDA) unveiled a plan to phase out the use of antimicrobials for the purpose of fattening chickens, pigs or other animals destined for human consumption. But the plan relies in part on voluntary industry cooperation, and advocates argue the government’s efforts are lagging behind even some industry players.
Here is the new full 78 pp. report to the President on antibiotic resistance (pdf).
This initiative — or its failure — is potentially a more important health issue than Obamacare, yet it will not receive 1/1000th of the attention. Without reliable antibiotics, a lot of now-routine operations would become a kind of lottery.
Here are previous MR posts on antibiotic resistance. I would note it is difficult to judge such a plan at the current level of detail. It is better than nothing, but any initial plan is going to be not nearly enough, relative to an ideal. By the way, Alex tells me there is also a British prize, discussed here.
Black ebola markets in everything
A black market for an Ebola treatment derived from the blood of survivors is emerging in the West African countries experiencing the worst outbreak of the virus on record, the World Health Organization said.
The United Nations health agency will work with governments to stamp out the illicit trade in convalescent serum, WHO Director-General Margaret Chan told reporters today in Geneva, where the organization is based. There is a danger that such serums could contain other infections and wouldn’t be administered properly, Chan said.
The WHO is encouraging the use of properly obtained serum to treat current patients and said last week it should be a priority. A third U.S. missionary worker who was infected with Ebola in Liberia and flown to the U.S. for medical care was treated with blood transfusions from another American who recovered from the virus last month. Doctors hope the virus-fighting antibodies in the blood help the 51-year-old physician, Rick Sacra.
There is more here, and for the pointer I thank John Chilton.
I am surprised this was admitted so quickly
The National Football League, which for years disputed evidence that its players had a high rate of severe brain damage, has stated in federal court documents that it expects nearly a third of retired players to develop long-term cognitive problems and that the conditions are likely to emerge at “notably younger ages” than in the general population.
There is more here, all of it a bit gruesome.
Further evidence for The Great Reset
Matt Yglesias writes:
…the Kaiser Family Foundation is out today with new reporting on employer benefit costs that reveals the slowdown is visible in this slice of the market. Premium costs rose by just 3 percent, a number much lower than they routinely rose by in the recent past. So how about those wage rises? Well — let’s just say there’s no evidence that they’re happening.
In other words, there is still downward pressure on real wages, even when we don’t always see real wage cuts.
This also means that the monetary policy argument “there can’t be a build up inflationary pressures because we don’t see real wages rising” is highly unreliable or at the very least a non sequitur (NB: I am not in fact extremely worried about inflationary pressures these days).
South Korea markets in everything
Fake casts for pretending you have an injured arm to evade having to help prepare holiday meals have become brisk sellers in South Korea ahead of the Chuseok festival.
“We have been selling this for 10 years now, but sales increased drastically starting last week,” said a sales manager at an online vendor who declined to be identified.
Both men and women were buying the bogus casts, he said.
During Chuseok, a three-day thanksgiving holiday, women traditionally do most of the work in preparing and cooking elaborate ceremonial dishes while the men of the family chat, drink and watch television.
The holiday gender divide is so entrenched that it has spawned the term “daughter-in-law holiday syndrome”, with many young women suffering post-holiday stress and fatigue.
But getting away with the phoney cast ruse may be difficult this year after several media outlets reported on brisk sales of the devices in the run-up to the holiday starting on Sunday.
Data from the Ministry of Gender, Equality, and Family in 2010 showed only 4.9 percent of people surveyed said both genders shared holiday chores, while the rest said women do most of the work.
There is more here, and for the pointer I thank David Lee.
What should we infer from Obamacare rate increases?
Robert Laszewski writes:
The 2015 rate increases have been largely modest. Does that prove Obamacare is sustainable? No. You might recall that on this blog months ago my 2015 rate increase prediction was for increases of 9.9%.
You might also recall my reason for predicting such a modest increase. With almost no valid claims data yet and the “3Rs” Obamacare reinsurance program, insurers have little if any useful information yet on which to base 2015 rates and the reinsurance program virtually protects the carrier from losing any money through 2016. I’ve actually had reports of actuarial consultants going around to the plans that failed to gain substantial market share suggesting they lower their rates in order to grab market share because they have nothing to lose with the now unlimited (the administration took the lid on payments off this summer) Obamacare reinsurance program covering their losses.
We won’t know what the real Obamacare rates will be until we see the 2017 rates––when there will be plenty of valid claim data and the Obamacare reinsurance program, now propping the rates up, will have ended.
The post has other interesting points.
Per capita Medicare spending is falling
I did not expect to be reading this within my lifetime, and yet here it is:
Medicare spending isn’t just lower than experts predicted a few years ago. On a per-person basis, Medicare spending is actually falling.
That is from Margot Sanger-Katz, there is more here. Do please note that the program still faces fiscal pressures, in part due to the ongoing rise in “n,” namely future program beneficiaries.
Why I am a relative optimist about Bolivia
1. Bolivia became a semi-stable democracy in the early 1980s and it has stayed that way.
2. For all the rhetoric to the contrary, the current regime is a mix of 1990s-era market-oriented reforms and Evo Morales. Probably you like one of these, though perhaps not both.
3. Many more Bolivian children go to school than before, and the incidence of malnutrition has been plummeting, with longer-run benefits for IQ. You will read many fabricated or non-causally-backed claims about the connection between inequality and growth, but for Bolivia I believe these arguments.
4. Bolivia has done so many things wrong in the past, there is a lot of low-hanging fruit through purely internal improvements. For instance the country is a fantastic tourist destination, but would not at this moment be experienced that way by mainstream American tourists, due to language, hotel, and infrastructure shortcomings. Eventually those problems can be and will be solved. Eventually.
5. Bolivia does not have much export exposure to China, and does not face much geopolitical risk.
6. Of all commodities, hydrocarbons may be relatively protected in price through the forthcoming global turmoil, because the Middle East implosion will make Bolivia’s current main resource more valuable.
7. Bolivia’s fiscal situation is surprisingly sound.
The three main reasons to be pessimistic about Bolivia are:
1. Most of their economic policy is quite bad, especially when it concerns the nationalization of foreign direct investment. The FDI future of Bolivia will be extremely unfavorable. The rhetoric and indeed the behavior of the government sometimes is like a villain from an Ayn Rand novel.
2. Their main trading partner is Brazil, a country which will have gone from eight percent growth to near-zero growth in but a few years time. Argentina is either the number two or number three trade partner, along with the U.S., depending on the year in question.
3. Bolivia hasn’t done that well in the past.
Of those three reasons, #1 probably matters a bit less than you might think, and #3 a bit more.
It is much debated in Bolivia whether corruption is going up or down. I believe it is going up, but partially for good reasons. For instance the construction sector is doing well, and construction tends to be corrupt in many countries, for reasons intrinsic to the activity itself (e.g., lots of big contracts, easy to claim invisible expenses, etc.). That means higher corruption but also a better corruption than the penny ante bribes of a shrinking economy.
Right now Bolivia is growing at a rate of above six percent.
Do wealth shocks affect the health of the elderly?
Hannes Schwandt of Princeton has a new paper (pdf) on this topic:
Do wealth shocks affect the health of the elderly in developed countries? The economic literature is sceptical about such effects which have so far only been found for poor retirees in poor countries. In this paper I show that wealth shocks also matter for the health of wealthy retirees in the US. I exploit the booms and busts in the US stock market as a natural experiment that generated considerable gains and losses in the wealth of stockholding retirees. Using data from the Health and Retirement Study I construct wealth shocks as the interaction of stock holdings with stock market changes. These constructed wealth shocks are highly predictive of changes in reported wealth. And they strongly affect health outcomes. A 10% wealth shock leads to an improvement of 2-3% of a standard deviation in physical health, mental health and survival rates. Effects are heterogeneous across physical health conditions, with most pronounced effects for the incidence of high blood pressure, smaller effects for heart problems and no effects for arthritis, diabetes, lung diseases and cancer. The comparison with the cross sectional relationship of wealth and health suggests that the estimated effects of wealth shocks are larger than the long-run wealth elasticity of health.
You can read more by Hannes Schwandt here.
China blackmail markets in everything
In Beijing, I met Benjamin Liebman, a professor at Columbia Law School, who has published a study on “malpractice mobs” in China. He told me that protests consistently extract more money from hospitals than legal proceedings do. Family members can even hire professional protesters. One report in Shenzhen mentioned an average price of fifty yuan a day for the service of a protester. The radiologist in Shanghai told me, “If your mother dies in the hospital, there will be an agency that comes to you and says, ‘We can help you. We can have twenty guys who can come to the hospital, blackmail them, and share fifty per cent of the profits.’ They’re very professional.”
The article, by Christopher Beam in The New Yorker, is interesting throughout.
Neil Harbisson is a cyborg
Or should that title read “Is Neil Harbisson a cyborg?”
Protruding from the back of Harbisson’s skull is a metal antenna that allows him to convert the frequencies for color into frequencies for sound and vice versa. He was born colorblind and the appendage has essentially given him a sixth sense to make up for what his vision lacks.
…Harbisson gets visibly dizzy when his antenna is off center. Moving it slightly to the left, he closed his eyes and said, “If I do this, I feel unbalanced…it does feel like a body part, an extension of a bone or something.” Even though the antenna is metal and has no nerve endings, Harbisson says he can feel when someone touches it, the same as a natural body part.
There is more:
Moon Ribas, Harbisson’s partner, has an extension she wears on her arm that makes her body vibrate when there’s an earthquake. (She plans to one day have it implanted under her skin.) As a choreographer, Ribas takes inspiration from nature and thought the extension would enhance her creativity. It syncs with an app that collects data on earthquakes around the world to make her body vibrate when there’s seismic activity (it happens frequently enough that she vibrated once during our interview).
But the appendage cannot be submerged in water, and neither can Neil’s. They are both hoping to update their devices so that in the future they can go swimming. “Then I will be able to perceive the colors in the ocean,” Harbisson says.
There is more here, including a photo. It is noted that security guards are sometimes unsympathetic to Harbisson, who is moving from Spain to New York, where he feels he will be seen as less unusual.
For a related pointer, I thank Samir Varma.
FDA Device Regulation
In the interests of length I had to sacrifice a few points in my WSJ review of Innovation Breakdown by Joseph Gulfo (excerpted on MR yesterday). In the review, I argued that the FDA could speed the approval of medical devices and reduce uncertainty by not reviewing directly but becoming a certifier of certifiers as is done in Europe.
In fact, a US model is already in place. OSHA, the Occupational Safety and Health, requires that a range of electrical products and materials meet certain safety standards but it outsources certification to Underwriters Laboratories and other Nationally Recognized Testing Laboratories. We could and should do the same for medical devices and for drugs. Indeed, if a device or drug is permitted in a developed, advanced economy such as in Europe, Australia and Japan then I see no reason why it ought not to be provisionally approved in the United States (and vice-versa).
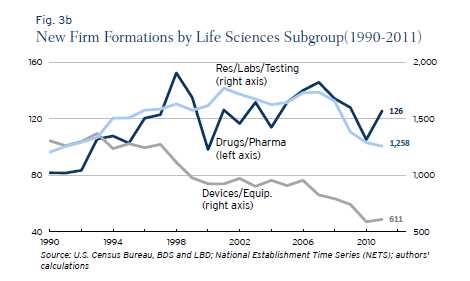
My paper with DiMasi and Milne showed that some FDA drug divisions appear to be much more productive than other divisions suggesting possibilities for substantial improvements if best practices were uniformly adopted. There also appear to be substantial differences between the regulation of drugs and devices especially in recent years. Ian Hathaway and Robert Litan have a new paper on Entrepreneurship and Job Creation in the U.S. Life Sciences Sector that shows that new firm creation in the medical device sector has fallen drastically since 1990 and far more than in the drug sector. Although there are likely many causes, the drop in the number of new firms is consistent with Gulfo’s experience of regulatory uncertainty and may suggest increases in regulatory cost for devices relative to drugs. Here is Hathaway and Litan:
The medical devices and equipment sector, on the other hand, saw new firm formations decline steadily and persistently between 1990 and 2011—falling by 695 firms or 53 percent during that period. Its share of new life sciences firms fell to 31 percent in 2011 from 50 percent in 1990. Unlike its life sciences sector counterparts, the decline in new firm formations in this segment appears to stretch beyond the cyclical effects of the Great Recession.
Innovation Breakdown
From my review today in the WSJ of Innovation Breakdown by Joseph Gulfo:
Yo is a smartphone app. MelaFind is a medical device. Yo sends one meaningless message: “Yo!” MelaFind tells you: “biopsy this and don’t biopsy that.” MelaFind saves lives. Yo does not. Guess which firm found it easier to put their product in consumers hands? Oy.
In “Innovation Breakdown: How the FDA and Wall Street Cripple Medical Advances,” Joseph Gulfo tells the tumultuous history of MELA Sciences, the company that invented MelaFind. When Dr. Gulfo joined the firm as president and CEO in 2004, the company’s brilliant team of scientists had spent many years and tens of millions of dollars to develop MelaFind, a “camera with a brain”—optical technology that would scan potential melanomas in multiple spectra and then, using sophisticated algorithms and large datasets, diagnose which were most likely to be cancerous.
MELA Sciences conducts an extensive clinical trial according to a protocol agreed on by the FDA and all looks good. After the clinical trial is completed, however, the FDA backs away from the protocol and comes out against MelaFind.
…The title of Dr. Gulfo’s book is “Innovation Breakdown” but “Innovator’s Breakdown” might have been more apt. The letter sent the author into survival mode. He battled the FDA, calmed investors, and defended against the lawsuit all while trying to keep the company afloat. Under stress, Dr. Gulfo’s health began to decline: He lost 29 pounds, his hair began to fall out, and the pain in his gut became so intense he needed an endoscopy. When his wife begged him to quit, he refused. They turned into roommates. “We were nothing more than cordial. I basically shut my wife out of my life,” he writes.
…The climax to this medical thriller comes when, in “the greatest 15 minutes of [his] life,” Dr. Gulfo delivers an impassioned speech, à la “Twelve Angry Men,” to the FDA’s advisory committee. The committee voted for approval, 8 to 7, and, perhaps with the congressional hearing in mind, the FDA approved MelaFind in September 2011.
It was a major triumph for the company, but Dr. Gulfo was beat. He retired from the company in June 2013—just in time to save his marriage.
Yet remarkably, given his experience, Mr. Gulfo writes that he still believes in a strong FDA. He argues in the book that better “leadership” and a few tweaks to existing rules can fix the problem. He’s wrong.
Compare MelaFind’s experience in the U.S. with its reception in Europe: MelaFind was submitted for marketing approval in Europe in May 2011. It was approved just five months later. One key reason for Europe’s efficient approval process is that European governments don’t review medical devices directly. Instead they certify independent “notified bodies” that specialize and compete to review new products. The European system works more quickly than the U.S. system, and there is no evidence that it results in reduced patient safety. Rather than tweak the current system, why doesn’t the U.S. just adopt the European model and call it a day? Our health and our economy would be better off for it.
Google’s Sergey Brin recently said that he didn’t want to be a health entrepreneur because “It’s just a painful business to be in . . . the regulatory burden in the U.S. is so high that I think it would dissuade a lot of entrepreneurs.” Mr. Brin won’t find anything in Dr. Gulfo’s book to persuade him otherwise. Until we get our regulatory system in order, expect a lot more Yo’s and not enough life-saving innovations.
In Defense of Johns
Jim Norton writing in Time:
…When I first began soliciting sex for money, it never occurred to me that some of them are possibly forced into prostitution or have abusive pimps. I must have known it deep down on an intellectual level, but hadn’t witnessed anything to confirm it.
Until I did.
The only experience I’ve had with an element of violence being present was driving on 48th Street in New York once and talking to a girl through my passenger window….As we were speaking, a van full of girls stopped and a guy who I assume was her pimp, bounced her across the hood of my car and threw her in the van.
This is why I’m a firm believer that prostitution should be legalized and pimps should be thrown down an elevator shaft.
Law enforcement stings designed to shame men who pay for sex are nothing more than the state blowing its own morality horn. Being a comedian who is single allows me a luxury most johns don’t have, which is the freedom to discuss the topic openly. And not from a ‘case study’ point of view, but from the honest point of view of someone who has spent the equivalent of a Harvard Law School education on purchasing sex.
By keeping prostitution illegal because we find it “morally objectionable,” we allow (or, more accurately, you allow) sex workers to constantly be put into dangerous situations. Studies have shown that rapes and STDs dropped drastically between 2003 and 2009 in Rhode Island after the state accidentally legalized it. The American Journal of Epidemiology showed that the homicide rate for prostitutes is 50 times higher than the next most dangerous job for a woman, working in a liquor store. You don’t need a Masters in sociology to understand it would be much safer for sex workers if they were permitted to work in places that provided adequate security. Legalizing prostitution would also alleviate the fear a sex worker may have about reporting the abusive behavior of a john out of fear of arrest.
…Give sex workers rights. Give johns a break.
Ebola and the FDA
The Telegraph reports:
The two American doctors who have caught Ebola have been treated with a new “secret serum” which could potentially save their lives.
…A source close to the Atlanta hospital, where Dr Brantly is being treated, told CNN: “Within an hour of receiving the medication, Brantly’s condition was nearly reversed. His breathing improved; the rash over his trunk faded away.”
One of his doctors reportedly described the events as “miraculous.”
…Dr Writebol was also administrated with the drug, which was transported to Liberia in a special sub-zero container. She showed a less remarkable recovery, but is hoped to travel to the US on Tuesday to continue her treatment.
According to CNN, the drug was developed by the biotech firm Mapp Biopharmaceutical, based in California. The patients were told that this treatment had never been tried before in a human being but had shown promise in small experiments with monkeys.
…health workers said drugs that could fight Ebola are not particularly complicated but pharmaceutical firms see no economic reason to invest in making them because the virus’ few victims are poor Africans.
Of course, pharmaceutical firms are not going to invest millions in getting a drug through FDA trials for a disease that has only killed a few thousand people since being discovered in 1976. Nevertheless, some people find this simple logic difficult to accept.
Prof John Ashton, Britain’s leading public health doctor, termed the “moral bankruptcy” of profit-driven drugs developers.
The logic of profit-driven drug developers is no different than the logic of profit driving automobile manufactures. It isn’t profitable to make cars for people who can’t afford them but the auto firms are rarely called morally bankrupt for not giving cars away to the poor. Moreover, it’s not at all obvious why the burden of producing unprofitable drugs should fall on the drug manufacturers. To the extent that there is an ethical case for developing drugs for the poor it’s a burden that falls on all of us.
As Eric Crampton notes there are at least two possible solutions. Either ensure at taxpayer expense a return on investment by subsidizing, offering prizes (as I suggested in Launching) or publicly investing in orphan drugs or
…ease up the FDA trials for drugs in this kind of category. Does it really make sense to mandate placebo trials for drugs hitting diseases with 60% fatality rates? We are condemning people to a very high risk of death for the sake of ensuring that there aren’t drug side effects and that the drugs are more effective than placebos (pretty easy to tell quickly where the fatality rate is otherwise 60%!).