Category: Medicine
The Demand for R&D is Increasing
In my TED talk I said that if India and China were as rich as the United States is today then the market for cancer drugs would be eight times larger than it is now. Larger markets, both in size and wealth, increase the incentive to invest in R&D. Larger markets save lives. As India and China become richer, they are investing more in R&D and investing more in educating the scientists and engineers who produce new ideas, new ideas that benefit everyone.
The WSJ reports on this trend:
Chipscreen’s drug, called chidamide, or Epidaza, was developed from start to finish in China. The medicine is the first of its kind approved for sale in China, and just the fourth in a new class globally. Dr. Lu estimates the research cost of chidamide was about $70 million, or about one-tenth what it would have cost to develop in the U.S.
…China’s spending on pharmaceuticals is expected to top $107 billion in 2015, up from $26 billion in 2007, according to Deloitte China. It will become the world’s second-largest drug market, after the U.S., by 2020, according to an analysis published last year in the Journal of Pharmaceutical Policy and Practice.
China has on-the-ground infrastructure labs, a critical mass of leading scientists and interested investors, according to Franck Le Deu, head of consultancy McKinsey & Co.’s pharmaceuticals and medical-products practice in China. “There’re all the elements for the recipe for potential in China,” he said.
We have much to gain from increased wealth in the developing world.
We ignore robot alarms, do we have to ignore robot alarms?
How many robot alarms are there anyway?
Every day, the bedside cardiac monitors threw off some 187 audible alerts. No, not 187 audible alerts for all the beds in the five ICUs; 187 alerts were generated by the monitors in each patient’s room, an average of one alarm buzzing or beeping by the bedside every eight minutes. Every day, there were about 15,000 alarms across all the ICU beds. For the entire month, there were 381,560 alarms across the five ICUs. Remember, this is from just one of about a half-dozen systems connected to the patients, each tossing off its own alerts and alarms.
And those are just the audible ones.
If you add the inaudible alerts, those that signal with flashing lights and text-based messages, there were 2,507,822 unique alarms in one month in our ICUs, the overwhelming majority of them false.
That is all from Bob Wachter, an interesting piece.
My conversation with Peter Thiel
The YouTube version is here, the podcast version is here.
I was very happy with how it turned out, as I deliberately set out not to copy the content of any of Peter’s other dialogues. You can learn how he thinks we will leave the “great stagnation,” whether the AI hype is justified, how he would boil his thought down to the smallest number of dimensions, whether NYC is over- or underrated, why globalization is likely to decline and what that means for different regions, the parts of the Bible which have influenced him most, “the Straussian Jesus,” to what age he thinks he will live, why Japan is special, how his German background matters, his favorite opening chess move, how and why company names matter, and even his favorite TV show, which he calls “schlocky.”
And much, much more, with commentary and questions from me throughout. A transcript is being prepared as well.
How a genre of music affects life expectancy of famous musicians in that genre
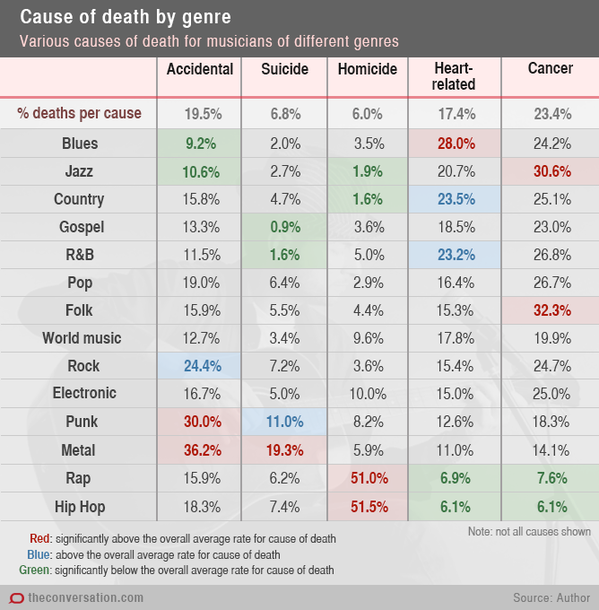
That is from Dianne Theodora Kenny, via Ted Gioia. Kenny notes:
For male musicians across all genres, accidental death (including all vehicular incidents and accidental overdose) accounted for almost 20% of all deaths. But accidental death for rock musicians was higher than this (24.4%) and for metal musicians higher still (36.2%).
Suicide accounted for almost 7% of all deaths in the total sample. However, for punk musicians, suicide accounted for 11% of deaths; for metal musicians, a staggering 19.3%. At just 0.9%, gospel musicians had the lowest suicide rate of all the genres studied.
Murder accounted for 6.0% of deaths across the sample, but was the cause of 51% of deaths in rap musicians and 51.5% of deaths for hip hop musicians, to date.
Beware selection, because of course most rap musicians aren’t dead yet. This problem will be more extreme, the younger is the genre. Another selection effect may be that getting killed, or dying in an unusual way, contributes to your fame.
The CRISPR revolution seems to be here, is this the coming of eugenics?
You will find a Qanta primer here. Here is an excerpt:
In the same month, separate teams of scientists at Harvard University and the Broad Institute reported similar success with the gene-editing tool. A scientific stampede commenced, and in just the past two years, researchers have performed hundreds of experiments on CRISPR. Their results hint that the technique may fundamentally change both medicine and agriculture.
Some scientists have repaired defective DNA in mice, for example, curing them of genetic disorders. Plant scientists have used CRISPR to edit genes in crops, raising hopes that they can engineer a better food supply. Some researchers are trying to rewrite the genomes of elephants, with the ultimate goal of re-creating a woolly mammoth. Writing last year in the journal Reproductive Biology and Endocrinology, Motoko Araki and Tetsuya Ishii of Hokkaido University in Japan predicted that doctors will be able to use CRISPR to alter the genes of human embryos “in the immediate future.”
Thanks to the speed of CRISPR research, the accolades have come quickly. Last year MIT Technology Review called CRISPR “the biggest biotech discovery of the century.” The Breakthrough Prize is just one of several prominent awards Doudna has won in recent months for her work on CRISPR; National Public Radio recently reported whispers of a possible Nobel in her future.
Even the pharmaceutical industry, which is often slow to embrace new scientific advances, is rushing to get in on the act. New companies developing CRISPR-based medicine are opening their doors. In January, the pharmaceutical giant Novartis announced that it would be using Doudna’s CRISPR technology for its research into cancer treatments. It plans to edit the genes of immune cells so that they will attack tumors.
How immediately will this come for ordinary use? Here is the big package of articles from Science. The Chinese already have done it with monkeys.
Here are my earlier remarks on eugenics. Here is a group of scientists calling for a moratorium on the technique, at least until rules can be established. Here are further articles on CRISPR. There are further comments here.
I believe the implications of all this — and its nearness to actual realization — have not yet hit either economics or the world of ideas more generally. This is probably big, big news.
Sentences to ponder
Smile! The Dentists Lose a Monopoly
Yesterday, the Supreme Court ruled (6:3) in North Carolina State Board of Dental Examiners v. FTC that the attempt of the state board of dental examiners to exclude nondentists from the practice of teeth whitening violated the Sherman antitrust act.
 The opinion, written by Justice Kennedy, is especially lucid. Here, from Kennedy, are the key facts:
The opinion, written by Justice Kennedy, is especially lucid. Here, from Kennedy, are the key facts:
Starting in 2006, the Board issued at least 47 cease-and desist letters on its official letterhead to nondentist teeth whitening service providers and product manufacturers. Many of those letters directed the recipient to cease “all activity constituting the practice of dentistry”; warned that the unlicensed practice of dentistry is a crime; and strongly implied (or expressly stated) that teeth whitening constitutes “the practice of dentistry.” App. 13, 15. In early 2007, the Board persuaded the North Carolina Board of Cosmetic Art Examiners to warn cosmetologists against providing teeth whitening services. Later that year, the Board sent letters to mall operators, stating that kiosk teeth whiteners were violating the Dental Practice Act and advising that the malls consider expelling violators from their premises.
These actions had the intended result. Nondentists ceased offering teeth whitening services in North Carolina.
The FTC then brought suit, arguing that the action was anti-competitive. The case raises constitutional issues because the states are allowed to violate the federal antitrust acts, as will inevitably happen in the ordinary use of their powers. The question then became whether the NC State Dental Board was invested with enough state authority to overcome the antitrust provisions. On the one hand, the principles of federalism say leave the states alone. On the other (Kennedy quoting Justice Stevens in Hoover v. Ronwin):
“The risk that private regulation of market entry, prices, or output may be designed to confer monopoly profits on members of an industry at the expense of the consuming public has been the central concern of . . . our antitrust jurisprudence.”
In my view, the majority deftly navigated the tradeoff. The court said that North Carolina can, without question, decide that teeth whitening is the practice of dentistry but they have to do so more or less explicitly–they can’t simply put the fox in charge of the hen-house by deferring the decision to the dentists.
In other words, the court raised the cost of rent-seeking. If the dentists want to monopolize the practice of teeth whitening they will have to make that case to the legislature and not rely on the unilateral actions of a board composed almost entirely of dentists and created for entirely different purposes.
As Kennedy put it in language reminiscent of bootleggers and baptists:
Limits on state-action immunity are most essential when the State seeks to delegate its regulatory power to active market participants, for established ethical standards may blend with private anticompetitive motives in a way difficult even for market participants to discern. Dual allegiances are not always apparent to an actor. In consequence, active market participants cannot be allowed to regulate their own markets free from antitrust accountability.
Addendum: I, along with a number of other GMU scholars, was part of an Institute for Justice BRIEF OF AMICI CURIAE SCHOLARS OF PUBLIC CHOICE ECONOMICS IN SUPPORT OF RESPONDENT. Congratulations are due to the excellent team at IJ, as the brief seems to have been influential.
By the way, the dissenting opinion (Alito, Scalia, Thomas) appears to accept the logic of our brief to an even greater extent, so much so that they shrug their shoulders at the rent seeking as business as usual (I especially enjoyed the dig at the FTC as also being subject to regulatory capture). Thus, the dissenters focused entirely on the federalism question. I respect that approach but I think that as federalism stands today, the majority’s balancing approach is likely to lead to better policy.
Totally conventional views which I hold
Most days on MR we try to bring you something new, whether it be a report or an opinion of ours. Even if it is not truly new, perhaps it is at least new relative to the discourse on most other web sites. We are reluctant to recycle old posts, even though I am still thinking about whether a lot of food tastes better when you eat it with your fingers.
But maybe telling you something conventional can be new in a way too. So here are a few totally conventional views which I hold, or still hold, but otherwise don’t bother reporting very often if at all:
1. Scott Walker and Jeb Bush are the most likely candidates to win the GOP nomination.
2. The GOP won’t try to repeal Obamacare, see #Syriza.
2b. Obamacare hasn’t made us healthier (yet?), but it has served as an inefficient form of wealth insurance for some lower-income groups. On net, the negative health consequences of the disemployment effects of the law could easily counterbalance the direct positive health care access effects. Imagine that, a health care reform that doesn’t even boost health. Given their utility functions, many of the law’s backers should be happy with it, but they shouldn’t think I am impressed with their numerous “victory lap” blog posts. Here is my 2009 post on what we should have done instead. I still think that, noting that I remain happy with the cost control parts of what was done.
3. The Supreme Court will rule against the current version of Obamacare and send the matter back to Congress. Confusion will result.
4. During the upward phase of the recovery, monetary policy just doesn’t matter that much.
5. We are still in the great stagnation, for the most part. But with nominal gdp well, well above its pre-crash peak, it is not demand-based “secular stagnation.” It just isn’t, I don’t know how else to put it. And the liquidity trap is still irrelevant and has been since about 2009.
6. There is modest good news on the wage front, but so far it doesn’t amount to a fundamental shift in regime. Following the monthly squiggles doesn’t tell us much. And since wage trouble dates from 1999 and arguably earlier, I don’t attribute much of it to debt overhang from the recession.
7. Edward Snowden is both a hero and a traitor.
8. Syriza still has to try to make a Greek economy work with roughly the same means their predecessors had. I don’t think they can do it, and I am sticking with my recent Grexit prediction, which by the way had an 18-month time horizon on it (see my earlier Twitter response to Felix Salmon).
9. No one knows what to do about ISIS or Putin. The latter is a bigger danger than the former. Confusion will result.
If you’re not excited, fine, that’s the point. The predictable is a kind of news, too. But hold on and come back, because tomorrow you might just hear more about remote-controlled, cyber cockroaches.
The economics of antibiotics
Ezekiel J. Emanuel writes:
The big problem is profitability. Unlike drugs for cholesterol or high blood pressure, or insulin for diabetes, which are taken every day for life, antibiotics tend to be given for a short time, a week or at most a few months. So profits have to be made on brief usage. Furthermore, any new antibiotics that might be developed to fight these drug-resistant bacteria are likely to be used very sparingly under highly controlled circumstances, to slow the development of resistant bacteria and extend their usefulness. This also limits the amount that can be sold.
The new and increasingly female path to the middle class
Right now the compass seems to be pointing in the direction of health care. That probably won’t change anytime soon:
In 1980, 1.4 million jobs in health care paid a middle class wage: $40,000 to $80,000 a year in today’s money. Now, the figure is 4.5 million.
The pay of registered nurses — now the third-largest middle-income occupation and one that continues to be overwhelmingly female — has risen strongly along with the increasing demands of the job. The median salary of $61,000 a year in 2012 was 55 percent greater, adjusted for inflation, than three decades earlier.
And it was about $9,000 more than the shriveled wages of, say, a phone company repairman, who would have been more likely to head a middle-class family in the 1980s. Back then, more than a quarter of middle-income jobs were in manufacturing, a sector long dominated by men. Today, it is just 13 percent.
The full story is here, by Searcey, Porter, and Gebeloff.
Health care cost control sentences to ponder
“I’m always curious when I read this ‘good news’ that health costs are moderating, because my health care costs go up significantly each year, and I think that’s a common experience,” said Mark Rukavina, president of Community Health Advisors in Massachusetts.
Um…how much time with Megan McArdle or Arnold Kling would it take to set him straight? The full story, of interest on other points too, is here.
Current research about vaccines and vaccination
From Harvard’s Kennedy Center:
…see the related article “Addressing Vaccine Hesitancy,” by report co-chairs Barry R. Bloom of the Harvard School of Public Health, Edgar Marcuse of the University of Washington and Seth Mnookin of MIT.
The beginning of this misinformation problem, researchers say, dates back to 1998, when a now-discredited scientific paper was published in Britain linking vaccines to autism, a link that was proven entirely false and even labeled “fraudulent.” A number of activists and some celebrities have adopted prominent anti-vaccine positions, and media and entertainment outlets have provided a platform for some of their views.
Despite the importance of this issue, little research has been done on how newer forms of technology and communication, including social media or video-sharing sites, influence health decision-making. And there are basic questions about the effectiveness of traditional public health campaigns. One of the most important studies to date is a 2014 paper in the journal Pediatrics, “Effective Messages in Vaccine Promotion: A Randomized Trial.” The researchers — Brendan Nyhan of Dartmouth College, Jason Reifler of the University of Exeter, Sean Richey of Georgia State University and Gary L. Freed of the University of Michigan — analyzed the results of a Web-based national survey of nearly 1,800 parents. After asking respondents about their own family health situations and beliefs, researchers then tested common public health communications strategies to promote vaccination: “(1) correcting misinformation, (2) presenting information on disease risks, (3) using dramatic narratives, or (4) displaying visuals to make those risks more salient or accessible.”
The study’s findings include:
- The data indicate that “pro-vaccine messages do not always work as intended and that the effectiveness of those messages may vary depending on parental attitudes toward vaccines.” In fact, there was “little evidence that messages emphasizing the risks of vaccine-preventable diseases were effective in promoting vaccination intent.”
- Further, the data show that a “dramatic narrative about measles and images of sick children” actually ended up increasing misperceptions about MMR.
- The study’s conclusion was unequivocal regarding traditional messaging: “None of the pro-vaccine messages created by public health authorities increased intent to vaccinate with MMR among a nationally representative sample of parents who have children age 17 years or younger at home. Corrective information reduced misperceptions about the vaccine/autism link but nonetheless decreased intent to vaccinate among parents who had the least favorable attitudes toward vaccines.”
By the way, Werner Troesken at the University of Pittsburgh will be publishing a new book on how American freedoms have allowed infectious diseases to spread, or so sounds the description. It is from University of Chicago press, due out in May.
BMI sentences to ponder
Table 1 shows that adding estimates from the literature suggests that economists have already explained 177% of the rise in average BMI.
That is from this new NBER paper, by Courtemanche, Pinkston, Ruhm, and Wehby, which seems to be one of the most careful studies to date. They do it right and then offer some more commonsensical conclusions:
A growing literature examines the effects of economic variables on obesity, typically focusing on only one or a few factors at a time. We build a more comprehensive economic model of body weight, combining the 1990-2010 Behavioral Risk Factor Surveillance System with 27 state-level variables related to general economic conditions, labor supply, and the monetary or time costs of calorie intake, physical activity, and cigarette smoking. Controlling for demographic characteristics and state and year fixed effects, changes in these economic variables collectively explain 37% of the rise in BMI, 43% of the rise in obesity, and 59% of the rise in class II/III obesity. Quantile regressions also point to large effects among the heaviest individuals, with half the rise in the 90th percentile of BMI explained by economic factors. Variables related to calorie intake – particularly restaurant and supercenter/warehouse club densities – are the primary drivers of the results.
Here is a much earlier ungated version of the paper, with differing numerical estimates, use with caution. A few related studies you will find here.
Is the “split benefit” a feasible way to reduce health care costs?
The excellent Kevin Lewis has pointed my attention to this paper by Robertson, Yokum, Sheth, and Joiner:. The idea will sound like common sense to an economist, namely give people some cash if they turn down special treatments of uncertain value. The funnier thing is, there is now some evidence it might actually work:
Traditional cost sharing for health care is stymied by limited patient wealth. The “split benefit” is a new way to reduce consumption of high-cost, low-value treatments for which the risk/benefit ratio is uncertain. When a physician prescribes a costly unproven procedure, the insurer could pay a portion of the benefit directly to the patient, creating a decision opportunity for the patient. The insurer saves the remainder, unless the patient consumes. In this paper, a vignette-based randomized controlled experiment with 1,800 respondents sought to test the potential efficacy of the split benefit. The intervention reduced the odds of consumption by about half. It did so regardless of scenario (cancer or cardiac stent), type of split (rebate, prepay, or health savings account), or amount of split (US$5,000 or US$15,000). Respondents viewed the insurer that paid a split as behaving fairly, as it preserved access and choice. Three-quarters of respondents supported such use in Medicare, which did not depend on political party affiliation. The reform is promising for further testing since it has the potential to decrease spending on low-value interventions, and thereby increase the value of the health care dollar.
My concern of course is that on a larger scale eventually this would be gamed, and faux treatment offers will be generated for the purpose of transferring wealth to patients, with doctors and hospitals, one way or the other, in on the act.
What will European QE look like? And will it work?
Claire Jones at the FT reports:
The European Central Bank is set to unveil a programme of mass bond buying next week to save the eurozone from deflation, but has bowed to German pressure to ensure that its taxpayers are not liable for any losses incurred on other countries’ debt.
This is not a surprise. Alen Mattich had a good Twitter comment:
How could you trust ECB promise to “do whatever it takes” if it doesn’t accept the risk of holding national sov debt on its books?
Guntram B. Wolff has an excellent, detailed analysis, worth reading in full, here is one bit:
So the purely national purchase of national sovereign debt would either leave the private creditors as junior creditors, or the national central bank has to accept negative equity. What would negative equity mean for a central bank? De facto it would mean that the national central bank, that has created euros to buy government debt, would have lost the claim on the government. It would still owe the euros it has created to the rest of the Eurosystem.(4) The Eurosystem could now either ask the national central bank to return that liability, which it is unable to do without a recapitalisation of its government. Or, the Eurosystem could decide to leave the claim standing relative to the national central bank. In that case, the loss made on the sovereign debt would de facto have been transferred to the Eurosystem. In other words, the attempt to leave default risk with the national central bank will have failed.
…Overall, this discussion shows that monetary policy in the monetary union reaches the limits of feasibility if the principle of joint and several liability at the level of the Eurosystem is given up.
An important open issue is whether the ECB could buy Greek bonds, given that they are up for restructuring and (presumably) the Bank cannot voluntarily relieve Greece of any debt (see Wolff’s discussion). There are plenty of rumors that Greece will indeed be excluded from any QE program, unless you imagine they settle things with the Troika rather more quickly than they are likely to. Yet a bond-buying program without Hellenic participation doesn’t seem so far from hurling an “eurozone heraus!” painted brick through their front window in the middle of the night.
Overall, shuffling assets and risk profiles between national monetary authorities and national fiscal authorities would seem to accomplish…nothing. Not buying up the debt of your biggest problem country also seems to accomplish nothing, in fact it is worth than doing nothing.
Here is my 2012 column on how the eurozone needs to agree on who is picking up the check. They still haven’t agreed! In the meantime, Grexit is a very real possibility, through deposit flight, no matter how badly Greek citizens may wish their country to stay in.
So, so far I am not so optimistic about this whole eurozone QE business, even though in principle I very much favor the idea. It is again a case of politics getting in the way of a problem which does indeed have a (partial) economic solution. The only way it (partially) works is if it (implicitly) bundles debt relief with higher rates of price inflation. Have a nice day.