Category: Medicine
Are quality-adjusted medical prices declining for chronic disease?
At least for diabetes care, the answer seems to be yes, according to Karen Eggleson, et.al.:
We analyze individual-level panel data on medical spending and health outcomes for 123,548 patients with type 2 diabetes in four health systems. Using a “cost-of-living” method that measures value based on improved survival, we find a positive net value of diabetes care: the value of improved survival outweighs the added costs of care in each of the four health systems. This finding is robust to accounting for selective survival, end-of-life spending, and a range of values for a life-year or, equivalently, to attributing only a fraction of survival improvements to medical care.
That is from a new NBER working paper. One way to read this paper is to be especially optimistic about medical progress, and also the U.S. health care system and furthermore the net contribution of science and medicine to economic growth. Another way to read this paper is to be especially pessimistic about human discipline and the ability to follow doctor’s orders.
The Economist covers Why Are the Prices So D*mn High?
The Economist does a very nice job covering Why Are the Prices So D*mn High.
Baumol’s earliest work on the subject, written with William Bowen, was published in 1965. Analyses like that of Messrs Helland and Tabarrok nonetheless feel novel, because the implications of cost disease remain so underappreciated in policy circles. For instance, the steadily rising expense of education and health care is almost universally deplored as an economic scourge, despite being caused by something indubitably good: rapid, if unevenly spread, productivity growth. Higher prices, if driven by cost disease, need not mean reduced affordability, since they reflect greater productive capacity elsewhere in the economy. The authors use an analogy: as a person’s salary increases, the cost of doing things other than work—like gardening, for example—rises, since each hour off the job means more forgone income. But that does not mean that time spent gardening has become less affordable.
It’s an implication of the Baumol effect that everyone ends up working in a low productivity industry!
The only true solution to cost disease is an economy-wide productivity slowdown—and one may be in the offing. Technological progress pushes employment into the sectors most resistant to productivity growth. Eventually, nearly everyone may have jobs that are valued for their inefficiency: as concert musicians, or artisanal cheesemakers, or members of the household staff of the very rich. If there is no high-productivity sector to lure such workers away, then the problem does not arise.
Misunderstanding the Baumol effect can lead to a cure worse than the “disease”:
These possibilities reveal the real threat from Baumol’s disease: not that work will flow toward less-productive industries, which is inevitable, but that gains from rising productivity are unevenly shared. When firms in highly productive industries crave highly credentialed workers, it is the pay of similar workers elsewhere in the economy—of doctors, say—that rises in response. That worsens inequality, as low-income workers must still pay higher prices for essential services like health care. Even so, the productivity growth that drives cost disease could make everyone better off. But governments often do too little to tax the winners and compensate the losers. And politicians who do not understand the Baumol effect sometimes cap spending on education and health. Unsurprisingly, since they misunderstand the diagnosis, the treatment they prescribe makes the ailment worse.
My only complaint is that the excellent reviewer has not followed our lead and called it the Baumol effect–cost disease is a misleading name!
Addendum: Other posts in this series.
What should I ask Masha Gessen?
I will be doing a Conversations with Tyler with her, no associated public event. What should I ask her? As always, I thank you all for your wisdom and counsel.
SlateStarCodex and Caplan on ‘Why Are the Prices So D*mn High?’
SlateStarCodex, whose 2017 post on the cost disease was one of the motivations for our investigation, says Why Are the Prices so D*mn High (now available in print, ePub, and PDF) is “the best thing I’ve heard all year. It restores my faith in humanity.” I wouldn’t go that far.
SSC does have some lingering doubts and points to certain areas where the data isn’t clear and where we could have been clearer. I think this is inevitable. A lot has happened in the post World War II era. In dealing with very long run trends so much else is going on that answers will never be conclusive. It’s hard to see the signal in the noise. I think of the Baumol effect as something analogous to global warming. The tides come and go but the sea level is slowly rising.
In contrast, my friend Bryan Caplan is not happy. Bryan’s basic point is to argue, ‘look around at all the stupid ways in which the government prevents health care and education prices from falling. Of course, government is the explanation for higher prices.’ In point of fact, I agree with many of Bryan’s points. Bryan says, for example, that immigration would lower health care prices. Indeed it would. (Aside: it does seem odd for Bryan to argue that if K-12 education were privately funded schools would not continue their insane practice of requiring primary school teachers to have B.A.s when in fact, as Bryan knows, credentialism has occurred throughout the economy)
The problem with Bryan’s critiques is that they miss what we are trying to explain which is why some prices have risen while others have fallen. Immigration would indeed lower health care prices but it would also lower the price of automobiles leaving the net difference unexplained. Bryan, the armchair economist, has a simple syllogism, regulation increases prices, education is regulated, therefore regulation explains higher education prices. The problem is that most industries are regulated. Think about the regulations that govern the manufacture of automobiles. Why do all modern automobiles look the same? As Car and Driver puts it:
In our hyperregulated modern world, the government dictates nearly every aspect of car design, from the size and color of the exterior lighting elements to how sharp the creases stamped into sheet metal can be.
(See Jeffrey Tucker for more). And that’s just design regulation. There are also environmental regulations (e.g. ethanol, catalytic converters, CAFE etc.), engine regulations, made in America regulations, not to mention all the regulations on the inputs like steel and coal. The government even regulates how cars can be sold, preventing Tesla from selling direct to the public! When you put all these regulations together it’s not at all obvious that there is more regulation in education than in auto manufacturing. Indeed, since the major increase in regulation since the 1970s has been in environmental regulation, which impacts manufacturing more than services, it seems plausible that regulation has increased more for auto manufacturing.
As an empirical economist, I am interested in testable hypotheses. A testable hypothesis is that the industries with the biggest increases in regulation have seen the biggest increases in prices over time. Yet, when we test that hypothesis as best we can it appears to be false. Remember, this does not mean that regulation doesn’t increase prices! It can and probably does it’s just that regulation is not the explanation for the differences in prices we see across industries. (Note also that Bryan argues that you don’t need increasing regulation to explain increasing prices, which is true, but I still need a testable hypotheses not an unfalsifiable claim.)
So by all means let’s deregulate, but don’t expect 70+ year price trends to reverse until robots and AI start improving productivity in services faster than in manufacturing.
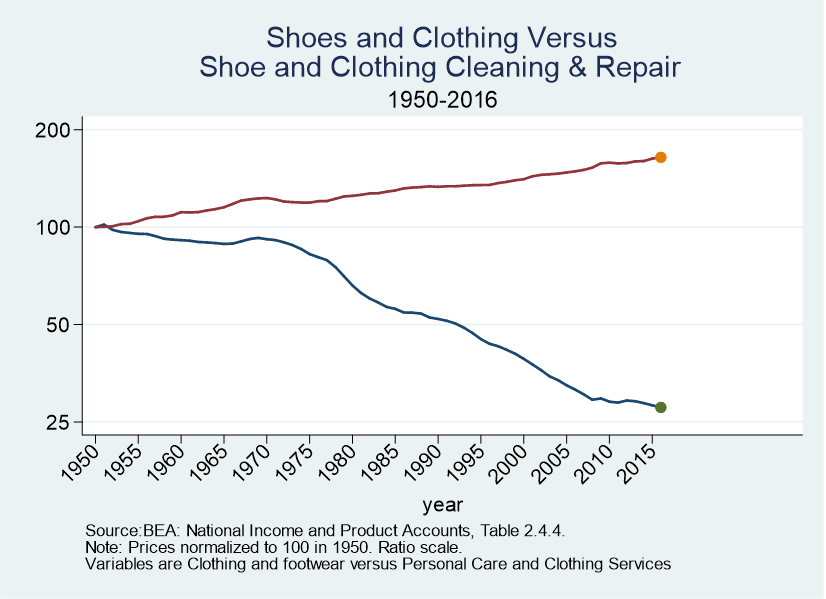
Let me close with this. What I found most convincing about the Baumol effect is consilience. Here, for example, are two figures which did not make the book. The first shows car prices versus car repair prices. The second shows shoe and clothing prices versus shoe repair, tailors, dry cleaners and hair styling. In both cases, the goods price is way down and the service price is up. The Baumol effect offers a unifying account of trends such as this across many different industries. Other theories tend to be ad hoc, false, or unfalsifiable.

Addendum: Other posts in this series.
Special Features of the Baumol Effect
I explained the Baumol effect in an earlier post based on Why Are the Prices So D*mn High?. In this post, I want to point out some special features of the Baumol effect that help to explain the data. Namely:
- The Baumol effect predicts that more spending will be accompanied by no increase in quality.
- The Baumol effect predicts that the increase in the relative price of the low productivity sector will be fastest when the economy is booming. i.e. the cost “disease” will be at its worst when the economy is most healthy!
- The Baumol effect cleanly resolves the mystery of higher prices accompanied by higher quantity demanded.

First, in the literature on rising prices it’s common to contrast massive increases in spending with little to no increases in quality, as for example, in contrasting education expenditures with mostly flat test scores (see at right). We have spent so much and gotten so little! Cui Bono? It must be teacher unions, administrators or the government!
All of that could be true but the Baumol effect predicts that more spending will be accompanied by no increase in quality. Go back to the classic example of the string quartet which becomes more expensive because labor in other industries increases in productivity over time. The price of the string quartet rises but does anyone expect that the the quality rises? Of course not. In the classic example the inputs to string quartet playing don’t change. The wages of the players rise because of productivity increases in other industries but we don’t invest any more real resources in string quartet playing and so we should not expect any increases in quality.
In just the same way, to the extent that greater spending on education, health care, or car repair is due to the rising opportunity costs of inputs we should not expect any increase in quality. (Note that increases in real resource use such as more teachers per student should result in increases in quality (and perhaps they do) but by eliminating the price increase portion of the higher spending we have eliminated a large portion of the mystery of higher spending with no increase in quality.)
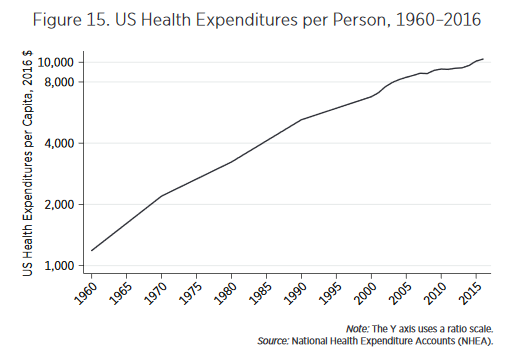 Second, explanations of rising prices that focus on bad things such as monopoly power or rent seeking tend to imply that price increases should be largest when the economy is doing poorly. In contrast, the Baumol effect predicts that increases in relative prices will be largest when the economy is booming. Consider health care. From news reports you might think that health care costs have gotten more “out of control” over time. In fact, the fastest increases in health care costs were in the 1960s. The graph at left is on a ratio scale so slopes indicate rates of growth and what one sees is that the growth rate of health expenditures per person is slowing. That might seem good but remember, from the Baumol point of view, the decline in relative price growth reflects slowing growth elsewhere in the economy.
Second, explanations of rising prices that focus on bad things such as monopoly power or rent seeking tend to imply that price increases should be largest when the economy is doing poorly. In contrast, the Baumol effect predicts that increases in relative prices will be largest when the economy is booming. Consider health care. From news reports you might think that health care costs have gotten more “out of control” over time. In fact, the fastest increases in health care costs were in the 1960s. The graph at left is on a ratio scale so slopes indicate rates of growth and what one sees is that the growth rate of health expenditures per person is slowing. That might seem good but remember, from the Baumol point of view, the decline in relative price growth reflects slowing growth elsewhere in the economy.
Third, holding all else equal, the only rational response to an ordinary cost increase is to substitute away from the good. But in many rising price sectors we see not only greater expenditures (driven by increased prices and inelastic demand) but also greater quantity demanded. As I showed earlier, for example, we have increased the number of doctors, nurses and teachers per capita even as prices have risen. John Cochrane correctly noted that this is puzzling but it’s a bigger puzzle for non-Baumol theories than for Baumol. For non-Baumol theories to explain increases in the quantity purchased, we need two theories. One theory to explain the increase in price (bloat/regulation etc.) and another theory to explain why, despite the increase in price, people are still purchasing more (e.g. income effect). The world is a messy place and maybe that is what is happening. But the Baumol effect offers a cleaner answer.
A Baumol increase in relative price is always accompanied by higher income so it’s much easier to explain how price increases can accompany increases in quantity as well as increases in expenditure. The Baumol story for increased purchase of medical care even as prices increase, for example, is no more mysterious than why people can take more leisure when wages increase–namely the higher wage means a higher income for any given hours and people choose to take some of this higher income in leisure. Similarly, higher productivity in say goods production increases income at any given production level and people choose to take some of this higher income in services.
Summing up, if we examine each sector–education, health care, the arts, etc.–on its own then there are always many possible explanations for why prices might be increasing. Many of these explanations have true premises–there are a lot of administrators in higher education, health care is highly regulated, lower education is government run. But, on closer inspection the arguments often don’t fit the data very well. Prices were increasing before administrators were important, health care is highly regulated but so is manufacturing, private education is also increasing in price, the arts are not highly regulated. It’s impossible to knock down each of these arguments in every industry, so there is always room for doubt. Indeed, the great difficult is that these factors often do result in higher costs and greater inefficiency but I believe those are predominantly level effects not effects that accumulate over time. Moreover, when one considers the rising price industries as a whole these explanations begin to look ad hoc. In contrast, the Baumol effect appears capable of explaining the pricing behavior of a wide variety of industries over a long period of time using a simple but powerful and unified theory.
Addendum: Other posts in this series.
The Baumol Effect
After looking at education and health care and doing a statistical analysis covering 139 industries, Helland and I conclude that a big factor in price increases over time in the rising price of skilled labor. Many industries use skilled labor, however, and even so prices decline so that cannot be a full explanation. Moreover, why is the price of skilled labor increasing? The Baumol effect answers both of these questions. In this post, I’ll explain the effect drawing from Why Are the Prices so D*mn High.
The Baumol effect is easy to explain but difficult to grasp. In 1826, when Beethoven’s String Quartet No. 14 was first played, it took four people 40 minutes to produce a performance. In 2010, it still took four people 40 minutes to produce a performance. Stated differently, in the nearly 200 years between 1826 and 2010, there was no growth in string quartet labor productivity. In 1826 it took 2.66 labor hours to produce one unit of output, and it took 2.66 labor hours to produce one unit of output in 2010.
Fortunately, most other sectors of the economy have experienced substantial growth in labor productivity since 1826. We can measure growth in labor productivity in the economy as a whole by looking at the growth in real wages. In 1826 the average hourly wage for a production worker was $1.14. In 2010 the average hourly wage for a production worker was $26.44, approximately 23 times higher in real (inflation-adjusted) terms. Growth in average labor productivity has a surprising implication: it makes the output of slow productivity-growth sectors (relatively) more expensive. In 1826, the average wage of $1.14 meant that the 2.66 hours needed to produce a performance of Beethoven’s String Quartet No. 14 had an opportunity cost of just $3.02. At a wage of $26.44, the 2.66 hours of labor in music production had an opportunity cost of $70.33. Thus, in 2010 it was 23 times (70.33/3.02) more expensive to produce a performance of Beethoven’s String Quartet No. 14 than in 1826. In other words, one had to give up more other goods and services to produce a music performance in 2010 than one did in 1826. Why? Simply because in 2010, society was better at producing other goods and services than in 1826.
The 23 times increase in the relative price of the string quartet is the driving force of Baumol’s cost disease. The focus on relative prices tells us that the cost disease is misnamed. The cost disease is not a disease but a blessing. To be sure, it would be better if productivity increased in all industries, but that is just to say that more is better. There is nothing negative about productivity growth, even if it is unbalanced.
In this post, I will discuss some implications of the fact that productivity is unbalanced. See the book for more discussion and speculation about why productivity growth is systematically unbalanced.
The Baumol effect reminds us that all prices are relative prices. An implication is that over time prices have very little connection to affordability. If the price of the same can of soup is higher at Wegmans than at Walmart we understand that soup is more affordable at Walmart. But if the price of the same can of soup is higher today than in the past it doesn’t imply that soup was more affordable in the past, even if we have done all the right corrections for inflation.
We can see this in the diagram at right. We have a two-good economy, Cars and Education. The production possibilities frontier shows all the combinations of Cars and Education that we can afford given our technology and resources at time 1 (PPF 1). Now suppose society chooses to consume the bundle of goods denoted by point (a). The relative price of Cars and Education is given by the slope of the PPF at that point. That price/slope tells us if we give up some education how many more cars can we get? In a market economy the price has to be given by the slope of the PPF because that is the only price at which people will willing consume the bundle of goods at point (a), i.e. it’s the equilibrium price.
Now at time 2, productivity has increased which means that with the same resources we can now have more of both goods. Productivity of Car production has increased more than that of Education production, however, so the curve shifts out more towards Cars than towards Education. Suppose society continues to consume Cars and Education in the same proportions, i.e. at point (b). The price of education must increase–and all that means is that if we give up a unit of education at point b we will get more cars than before which is the same as saying that if we want more education at point b we must give up more cars than before, i.e. the price has increased.
Notice, however, that although the price of education has increased, education is not less affordable. Indeed, at point (b) we are consuming more of both goods–broadly speaking this is exactly what has happened–namely, the price of education has increased and we now consume more of it than ever before.
When we recognize that all prices are relative prices the following simple yet deep facts follow:
- If productivity increases in some industries more than others then, ceteris paribus, some prices must increase.
- Over time, all real prices cannot fall.
In Figure 22 the economy moves from point (a) to point (b). If we graph the same transition over time it will look something like Figure 23.
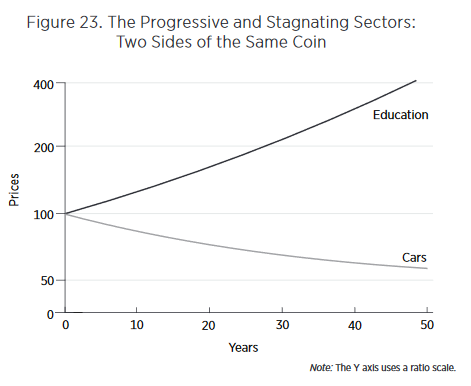
Looking at such graphs, our attention naturally is drawn to the rising cost of education. Why are costs rising so quickly? Entranced by such graphs, we may enter into a detailed analysis of the special factors of education—regulation, unionization, government purchases, insurance, international trade, and so forth—to try to explain the dramatic increase in costs. Yet the rising costs in the education sector are simply a reflection of increased productivity in the car sector. Thus, another deep lesson of the Baumol effect is that to understand why costs in the stagnant sector are rising, we must look away from the stagnating sector and toward the progressive sector.
Finally, there is one other addition to the Baumol effect which is not often recognized but worth drawing attention to. In Figure 22, I assumed that preferences were such that people wanted to consume the same ratio of goods over time so we moved from point (a) to point (b). But suppose that as we get wealthier we get tired of more cars and would like relatively more education so we move towards point (d). As we move from point (b) to point (d) we are taking resources away from car production, resources which were probably well-suited to making cars, and instead moving them towards education where they are probably less well suited. As a result as we move from point (b) to point (d) we are driving up the price of education as we try to turn auto workers into teachers. In this case, the Baumol effect gets magnified. We could alternatively move from point (b) to point (c) which would turn teachers into less productive auto workers thus driving down the price of education (i.e. increasing the price of cars). Thus, depending on preferences, the Baumol effect can be magnified or ameliorated.
As a society it appears that with greater wealth we have wanted to consume more of the goods like education and health care that have relatively slow productivity growth. Thus, preferences have magnified the Baumol effect.
Next week, I will wrap up the discussion by explaining some features of the data that the Baumol effect fits much better than do other theories.
Addendum: Other posts in this series.
The Tremendous Value of Increases in Life Expectancy
In this post I shall argue two things which together may confuse people. First, that life expectancy is so valuable that the money the US spends on healthcare relative to Europe could be well spent. Second that the extra spending is not in fact due to higher quality and does not explain rising prices over time.
What explains rising prices in some sectors of the economy? A common argument, at least from economists, is that there may be unmeasured improvements in quality. I don’t think that there have been marked improvements in quality in education so that argument doesn’t get off the ground (see my earlier post and the book for evidence). But health care quality has increased. Moreover, the value of life is so high that the improvements in quality could justify the cost increases. Here from Why Are The Prices So D*mn High is a back of the envelope calculation:
The United States spends about 5 percent more of GDP on health-care than do other developed countries. US GDP is almost $20 trillion, so 5 percent is approximately $1 trillion. The US population is 325 million, so the United States spends an extra $3,000 per person each year on healthcare. Is the expense worthwhile?
A value of a statistical life-year of around $200,000 is a mid-range, widely used estimate in the United States. Thus, if the extra US spending generated an extra $3,000 per $200,000 of a life-year, it would pay for itself. In other words, for the extra US spending to be worthwhile it must generate 3,000/200,000 × 365 = 5.45 extra days of statistical life, and, of course, it must do so every year. In recent years, life expectancy in the United States has increased by about 52 days a year. Thus, a little more than 10 percent of the increase in actual life expectancy must be a result of the extra US spending for that spending to be worthwhile. That hardly appears impossible. It’s also not impossible that the increase in life expectancy was not caused by the extra spending.
The bottom line is that the value of life is so high that US levels of spending could be worthwhile, but the high value of life and the difficulty of measuring the effectiveness of healthcare makes the question impossible to answer with certainty.
Nevertheless,I don’t think the increases in quality explain the increases in cost:
…even if the spending on healthcare is well justified by the improvements in life expectancy, it does not follow that the cause of higher spending is the improvement in life expectancy. As with education, many of the increases in life expectancy come from better knowledge, which does not necessarily cost more to use. It does not cost much more to treat an infection with antibiotics than with bloodletting; perhaps it costs less. We do use more technology in healthcare than in previous years—this includes computerized tomography (CT) scanners, magnetic resonance imaging (MRI) systems, and positron emission tomography (PET). Technology, however, is falling in price. At some point one would expect that decreases in the cost of existing technologies would overwhelm increases in costs owing to the introduction of new technologies. As with education, it would be peculiar if the only place in which technology raised costs was in healthcare (but see Joseph P. Newhouse for a strong argument that healthcare costs are driven by technology.)
Let’s put this argument more generally. Most increases in quality *over time* are similar to increases in productivity, i.e. A in A*f(K,L), an unpriced factor. Computers today are much higher quality than in the past. Indeed, so much so that today’s computers couldn’t be bought at any price not that long ago but we don’t pay more because what makes them higher quality is general knowledge.
In my view, most quality increases over time are due to improvements in knowledge. In other words, quality increases over time are much more about better recipes than better cooks. As a result, at a given point in time, higher quality is associated with higher prices but over time higher quality is more often associated with *lower* prices. Thus, in general, higher quality is not a good explanation for higher prices over time.
Tomorrow: The Baumol Effect.
Addendum: Other posts in this series.
Physician and Nurse Incomes Have Increased Tremendously
 There has been a lot of ink spilled over the rising cost of health care and in Why Are the Prices So D*mn High? Helland and I do not cover every theory and cannot satisfy every objection. Our goal is more modest. We can say that one major factor in rising health care costs is the rising price of skilled labor.
There has been a lot of ink spilled over the rising cost of health care and in Why Are the Prices So D*mn High? Helland and I do not cover every theory and cannot satisfy every objection. Our goal is more modest. We can say that one major factor in rising health care costs is the rising price of skilled labor.

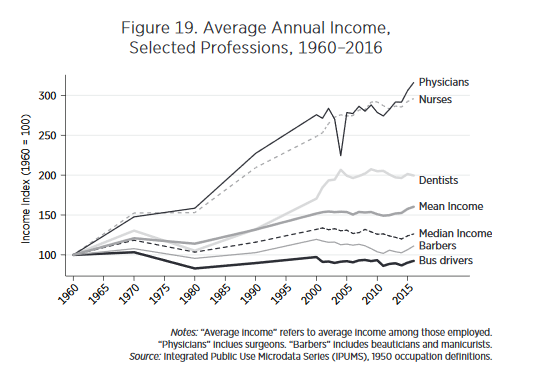
We argue that there is a direct, obvious, and measurable cause of higher costs in healthcare—namely, the price of skilled labor. No profession other than physicians has seen such large increases in incomes over the past 50 years. Figure 19 shows the real income of physicians from 1960 to 2016, indexed to 100 in 1960. Since 1960 the real income of physicians has increased by a factor of three. By comparison, barbers and bus drivers have seen essentially no increase in real incomes. Median incomes are up only modestly whereas mean incomes, which are pulled up by outliers, are up by only 50 percent.
Moreover, nurse incomes have risen in lock-step with those of physicians.
At the same time, we have hired more physicians and more nurses per capita. As Figure 20 shows since 1960 the number of physicians and the number of nurses has more than doubled.
With more physicians and more nurses each making more, it’s not surprising that the cost of medical care would increase.
Addendum: Other posts in this series.
Chernobyl
 Chernobyl, HBO’s taut 5-part mini-series, is excellent and it sticks close to the facts (although one female character played by Emily Watson is clearly made up). By all accounts, the series accurately represents life in the former Soviet Union and through a variety of means from color palette to casting and dialogue it does a remarkable job at capturing the political economy. One thing I learned (so far, it hasn’t all appeared yet) is that it could have been much, much worse but the Russians avoided the worst scenario with a combination of bravery, smarts and luck.
Chernobyl, HBO’s taut 5-part mini-series, is excellent and it sticks close to the facts (although one female character played by Emily Watson is clearly made up). By all accounts, the series accurately represents life in the former Soviet Union and through a variety of means from color palette to casting and dialogue it does a remarkable job at capturing the political economy. One thing I learned (so far, it hasn’t all appeared yet) is that it could have been much, much worse but the Russians avoided the worst scenario with a combination of bravery, smarts and luck.
The number of cancer deaths from Chernobyl appears to be quite low. The WHO estimated an additional 9,335 deaths with about half of those coming from workers and nearby residents and other half more distant impacts, other estimates are higher. More recent analysis, however, suggests that Chernobyl and its aftermath had relatively small but significant effects across a large number of people. Here are two recent papers:
Chernobyl’s Subclinical Legacy: Prenatal Exposure to Radioactive Fallout and School Outcomes in Sweden by Almond, Edlund and Palme.
Abstract: We use prenatal exposure to Chernobyl fallout in Sweden as a natural experiment inducing variation in cognitive ability. Students born in regions of Sweden with higher fallout performed worse in secondary school, in mathematics in particular. Damage is accentuated within families (i.e., siblings comparison) and among children born to parents with low education. In contrast, we detect no corresponding damage to health outcomes. To the extent that parents responded to the cognitive endowment, we infer that parental investments reinforced the initial Chernobyl damage. From a public health perspective, our findings suggest that cognitive ability is compromised at radiation doses currently considered harmless.
and The long-run consequences of Chernobyl: Evidence on subjective well-being, mental health and welfare by Danzer and Danzer.
Abstract: This paper assesses the long-run toll taken by a large-scale technological disaster on welfare, well-being and mental health. We estimate the causal effect of the 1986 Chernobyl catastrophe after 20 years by linking geographic variation in radioactive fallout to respondents of a nationally representative survey in Ukraine according to their place of residence in 1986. We exclude individuals who were exposed to high levels of radiation—about 4% of the population. Instead, we focus on the remaining majority of Ukrainians who received subclinical radiation doses; we find large and persistent psychological effects of this nuclear disaster. Affected individuals exhibit poorer subjective well-being, higher depression rates and lower subjective survival probabilities; they rely more on governmental transfers as source of subsistence. We estimate the aggregate annual welfare loss at 2–6% of Ukraine’s GDP highlighting previously ignored externalities of large-scale catastrophes.
Hat tip: Jennifer Doleac and Wojtek Kopczuk.
Why Are the Prices So D*MN High?
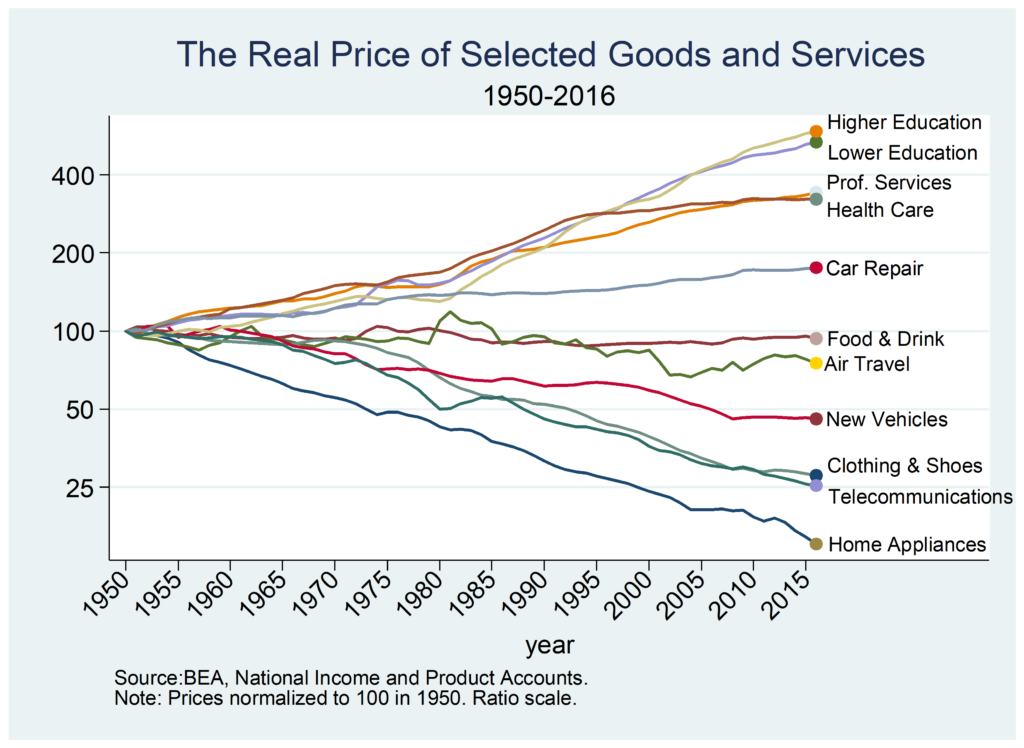
Why have some prices increased since 1950 by a factor of four while other prices have decreased by a factor of four? Technology is making so many goods and services much cheaper than in the past–that seems to be the normal situation–so why do some industries seem not only to be not progressing but actually retrogessing? As Scott Alexander put it, why are some industries so weird?
Those are the questions that motivated my latest piece, a short book with Eric Helland just released by the Mercatus Center titled, Why are the Prices so D*mn High?
In approaching this question I had some ideas in mind. I assumed that regulation, bloat and bureaucracy, monopoly power and the Baumol effect would each explain some of what is going on. After looking at this in depth, however, my conclusion is that it’s almost all Baumol effect. That conclusion radically changes one’s evaluation of price increases and decreases over the long run and it changes what, if anything, one might try to do to address such price changes.
Next week I will examine some of the evidence that pushes me towards this verdict. I’ll also take a closer look at the Baumol effect, which is mistakenly called the cost disease.
Let’s note here, however, what we need to explain. For the most part, we don’t see quick, big changes in prices that then level off. That in itself is interesting since policy tends to be discontinuous. We might expect a big regulation, for example, to cause a big increase in prices as industries adjust but then growth should return to normal. Instead, what we see and need to explain is slow, steady rising relative prices that happens over decades. Indeed, in some cases, such as education, prices have been increasing faster than average for more than a century! Puzzle over that over the long weekend. More next week!
Addendum: Other posts in this series.
My Conversation with Ezekiel Emanuel
Very much a fun one, here is the audio and transcript, here is part of the opening summary:
Do we overrate the importance of doctors? What’s the importance of IQ versus EQ in the practice of medicine? What are the prospect for venture capital in biotech? How should medical training be changed? Why does he think the conventional wisdom about a problem tends to be wrong? Would immortality be boring? What would happen if we let parents genetically engineer their kids?
Tyler questions Emanuel on these topics and more, including the smartest thing his parents did while raising him, whether we have right to medical self-defense, healthcare in low- versus high-trust institutions, and much more.
Here is one excerpt:
COWEN: How can we improve medical education?
EMANUEL: Cut it down. Make it shorter.
COWEN: Cut it down? Why does that make it better? Or does it just make it cheaper?
EMANUEL: No, I think it will make it better. So, we have a lot of memorization, a lot of . . . So, let’s go back to the start. The four years of medical school: two years of preclinical in the classroom learning about biochemistry, genetics, anatomy, microbiology; and the two years of clinical time in the hospital, on the wards.
That dates from 1910. We haven’t really updated it much, except in this one way: we’ve cut down the preclinical time because — less of it — and it changes so fast, by the time you learn it in medical school, get out as a doctor, it’s out of date, A; and B, it’s more or less irrelevant to managing most patients…
And then, by the way, in med school, spending your time in a hospital is not the future. The future of American medicine is out of the hospital. So we need more rotations, more experiences for students out of the hospital.
No med school has made that big shift, and those are the shifts that are going to have to happen over the next 15 or so years.
And:
COWEN: Is there a right to medical self-defense that should override FDA bans on drugs and medical devices? I want to try something that’s not approved —
EMANUEL: No. I don’t like that.
COWEN: I’m saying it’s my body. But why don’t you like it?
EMANUEL: No, no, no, no, no, no, no, no, no, Tyler.
Finally:
COWEN: Now, you’ve written a much-misunderstood article about how hard you would try yourself to live past the age of 75. Would not the suspense of world and national history always keep you wanting a bit more extra time?
So, say I’m 75. I’ve decided I agree with you, but the NBA Finals aren’t over yet. I want to see game seven. I want the Mueller report to come out. Isn’t there always something?
And then, it’s kind of intransitivity of indifference. Every day there’s something, and you just keep on hanging on, even if one accepts your arguments in the abstract. Can you talk me out of that?
EMANUEL: No, no, Tyler, I think you’re exactly right. That’s why people do hang on. It’s because . . . you know, so I talked to my father, who — he says, “Zeke, you’re absolutely right. I’ve become slower, physically slower, mentally slower. My life” . . . what ends up happening is your life cones down, and you begin to overvalue certain small things. Like the NBA Finals. Like what’s in the Mueller report.
We all know, from any cosmic standpoint — even not a cosmic standpoint, just a 2,000-foot standpoint — most of those things are not irrelevant. It’s really cool to know.
You often ask — and this happens to me all the time. I teach undergraduates. Pretty smart undergraduates. Very smart undergraduates. MBA students, nurses, doctors, right? They have no understanding of history. So, whoever finishes in the NBA Finals, in five years, people have forgotten.
Recommended, interesting throughout.
Why Do Experiments Make People Uneasy?
People were outraged in 2014 when Facebook revealed that it had run “psychological experiments” on its users. Yet Facebook changes the way it operates on a daily basis and few complain. Indeed, every change in the way that Facebook operates is an A/B test in which one arm is never run, yet people object to A/B tests but not to either A or B for everyone. Why?
In an important and sad new paper Meyer et al. show in a series of 16 tests that unease with experiments is replicable and general. The authors, for example, ask 679 people in a survey to rate the appropriateness of three interventions designed to reduce hospital infections. The three interventions are:
-
Badge (A): The director decides that all doctors who perform this procedure will have the standard safety precautions printed on the back of their hospital ID badges.
-
Poster (B): The director decides that all rooms where this procedure is done will have a poster displaying the standard safety precautions.
- A/B: The director decides to run an experiment by randomly assigning patients to be treated by a doctor wearing the badge or in a room with the poster. After a year, the director will have all patients treated in whichever way turns out to have the highest survival rate.
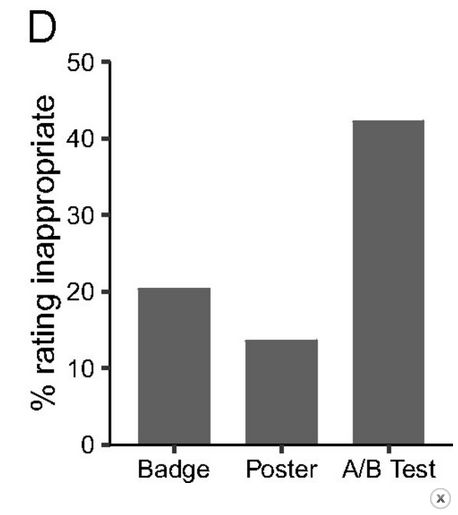 It’s obvious to me that the A/B test is much better than either A or B and indeed the authors even put their thumb on the scales a bit because the A/B scenario specifically mentions the positive goal of learning. Yet, in multiple samples people consistently rate the A/B scenario as more inappropriate than either A or B (see Figure at right).
It’s obvious to me that the A/B test is much better than either A or B and indeed the authors even put their thumb on the scales a bit because the A/B scenario specifically mentions the positive goal of learning. Yet, in multiple samples people consistently rate the A/B scenario as more inappropriate than either A or B (see Figure at right).
Why do people do this? One possibility is that survey respondents have some prejudgment about whether the Badge or Poster is the better approach and so those who think Badge is better rate the A/B test as inappropriate as do those who think Poster is better. To examine this possibility the authors ask about a doctor who prescribes all of his patients Drug A or all of them Drug B or who randomizes for a year between A and B and then chooses. Why anyone would think Drug A is better than Drug B or vice-versa is a mystery but once again the A/B experiment is judged more inappropriate than prescribing Drug A or Drug B to everyone.
Maybe people don’t like the idea that someone is rolling dice to decide on medical treatment. In another experiment the authors describe a situation where some Doctors prescribe Drug A and others prescribe Drug B but which drug a patient receives depends on which doctor is available at the time the patient walks into the clinic. Here no one is rolling dice and the effect is smaller but respondents continue to rate the A/B experiment as more inappropriate.
The lack of implied consent does bother people but only in the explicit A/B experiment and hardly ever in the implicit all A or all B experiments. The authors also show the effect persists in non-medical settings.
One factor which comes out of respondent comments is that the experiment forces people to reckon with the idea that even experts don’t know what the right thing to do is and that confession of ignorance bothers people. (This is also one reason why people may prefer pundits who always “know” the right thing to do even when they manifestly do not).
Surprisingly and depressingly, having a science degree does not solve the problem. In one sad experiment the authors run the test at an American HMO. Earlier surveys had found huge support for the idea that the HMO should engage in “continuous learning” and that “a learning health system is necessary to provide safe, effective, and beneficial patient-centered care”. Yet when push came to shove, exactly the same pattern of accepting A or B but not an A/B test was prevalent.
Unease with experiments appears to be general and deep. Widespread random experiments are a relatively new phenomena and the authors speculate that unease reflects lack of familiarity. But why is widespread use of random experiments new? In an earlier post, I wrote about ideas behind their time, ideas that could have come much earlier but didn’t. Random experiments could have come thousands of years earlier but didn’t. Thus, I think the authors have got the story backward. Random experiments generate unease not because they are new, they are new because they generate unease.
Our reluctance to conduct experiments burdens us with ignorance. Understanding and overcoming experiment-unease is an important area for experimental research. If we can overcome our unease.
Bhutan’s prime minister spends his weekends as a surgeon
Take that Adam Smith!:
Dr Lotay Tshering was one of Bhutan’s most highly regarded doctors before he entered politics last year, and while his prime ministerial duties occupy him during the week, on weekends he returns to the hospital as a way to let off steam.
“Some people play golf, some do archery, and I like to operate,” Tshering told AFP as he tended to patients one Saturday morning at Jigme Dorji Wangchuck national referral hospital, describing his moonlighting medical work as a “de-stresser”.
“I will continue doing this until I die and I miss not being able to be here every day,” he added. “Whenever I drive to work on weekdays, I wish I could turn left towards the hospital.”
Far from finding the two roles hard to juggle, Tshering said he had found that there was unexpected crossover between prime minister and surgeon. “At the hospital I scan and treat patients. In the government, I scan the health of policies and try to make them better,” he said. He has also put healthcare reform at the heart of his political agenda.
Here is the full story, via Anecdotal.
How Much Did Physicians Drive the Opioid Crisis?
It’s well known that the opioid crisis started with prescription abuse but how much abuse was driven by patients who fooled their physicians and how much was driven by physicians who responded to monetary incentives with a nod and a wink? Molly Schnell provides some evidence which even a hard headed rationalist like myself found startling.
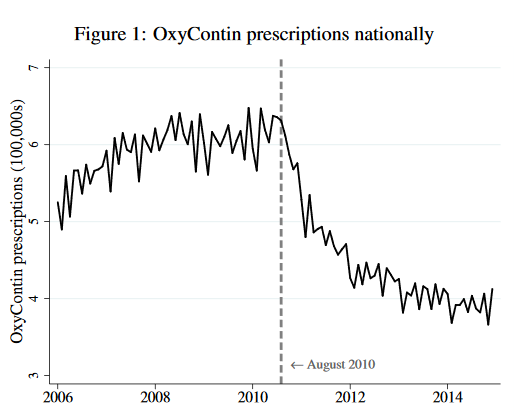 In August of 2010, Purdue Pharma replaced old OxyContin with a new, anti-abuse version of OxyContin. The new version was just as good at reducing pain as the old but it was more difficult to turn it into an injectable to produce a high. If physicians are altruists who balance treating their patient’s pain against their fear of patient addiction and downstream abuse then they should increase their prescriptions of new Oxy. From the point of view of health, the new Oxy is simply a better drug and with less abuse to worry about altruistic physicians should be more willing on the margin to prescribe Oxy to reduce pain. So what happened? Prescriptions for Oxy fell immediately and dramatically when the better version was released.
In August of 2010, Purdue Pharma replaced old OxyContin with a new, anti-abuse version of OxyContin. The new version was just as good at reducing pain as the old but it was more difficult to turn it into an injectable to produce a high. If physicians are altruists who balance treating their patient’s pain against their fear of patient addiction and downstream abuse then they should increase their prescriptions of new Oxy. From the point of view of health, the new Oxy is simply a better drug and with less abuse to worry about altruistic physicians should be more willing on the margin to prescribe Oxy to reduce pain. So what happened? Prescriptions for Oxy fell immediately and dramatically when the better version was released.
Now, to be fair to the physicians, patients who wanted to abuse Oxy stopped demanding it after the new version was released and physicians might not have realized how many of their prescriptions were being abused or sold on the secondary market. The aggregate data, which is a combination of supply and demand shifts, can mask individual physician behavior. Schnell, however, has data on the prescribing behavior of about 100,000 individual physicians who prescribed opioids.
Schnell finds that nearly a third of physicians behaved exactly as the altruism theory predicts. Namely, when new Oxy was released these altruistic physicians increased their prescriptions of Oxy and they maintained or reduced their prescriptions of other opioids. In fact, the median altruistic physician doubled their prescriptions of the new and improved Oxy. But almost 40% of physicians in Schnell’s sample behaved in a decidedly non-altruistic manner. Beginning in August of 2010, these non-altruistic physicians halved their prescriptions of new and improved Oxy and increased their prescriptions of other opioids. It’s difficult to see how attentive and altruistic physicians could decrease their demand for a better drug.
Schnell also finds that some parts of the country had fewer altruistic physicians and the consequences are evident in mortality statistics:
…. these differences in physician altruism across commuting zones translate into significant differences in mortality across locations…a one standard deviation increase in low-altruism physicians is associated with a 0.33 standard deviation increase in deaths involving drugs per capita. While this association is reduced conditional on observable commuting zone characteristics (including race, age, education, and income profiles), a significant and large association between the share of low-altruism physicians and drug-related mortality remains. Furthermore…this relationship persists even conditional on the number of opioid prescriptions, suggesting that the association is driven by the allocation of prescriptions introduced by low-altruism physicians rather than simply the quantity.
The less-altruistic physicians increased prescriptions for other opioids after new Oxy was introduced but perhaps even this was better than the non-prescription alternatives like heroin and street fentanyl. Indeed, Alpert, Powell and Pacula show that the introduction of improved Oxy led to more deaths because people switched to more dangerous, illegal alternatives. So was it a bad idea to introduce a better drug? Maybe, but if new Oxy had been introduced earlier perhaps fewer people would have been addicted, leading to less demand for illegal markets later. Thus, static and dynamic effects may differ. The economics of dual use goods is complicated.
Did rising health care expenditures damage the U.S. savings rate?
Maybe so:
The U.S. saving rate declined by 8 percent between 1980 and 2009. We document that the decline can be explained by rising health expenditures. Using exogenous variation in medical expenses generated by FDA drug approvals, we document that a 1 percentage point increase in health expenditure generated a decline in saving rate of 0.9 percentage points. We then estimate a model of household decisions to evaluate the mechanisms behind the decline. We find that the rise in health expenses and drop in saving rate are driven by progress in health technology, reduction in co‐payment rates, and improvements in income processes.
That is by Yi Chen, Maurizio Mazzocco, and Béla Személy, via the excellent Kevin Lewis.