Marginal Garfield
Marginal Garfield generates an original Garfield cartoon every day based on posts from Marginal Revolution! Here is the first strip. You can guess the post. Is there now any reason to come to MR? What a world.
You can also check out Rationalist Garfield which pulls from Less Wrong.
We thank Tim Hwang.
Physician Incomes and the Extreme Shortage of High IQ Workers
Physician incomes are extraordinarily high in the United States. A new NBER paper finds that U.S. physicians earn roughly two to four times as much as their counterparts in Canada, the Netherlands, and Sweden.
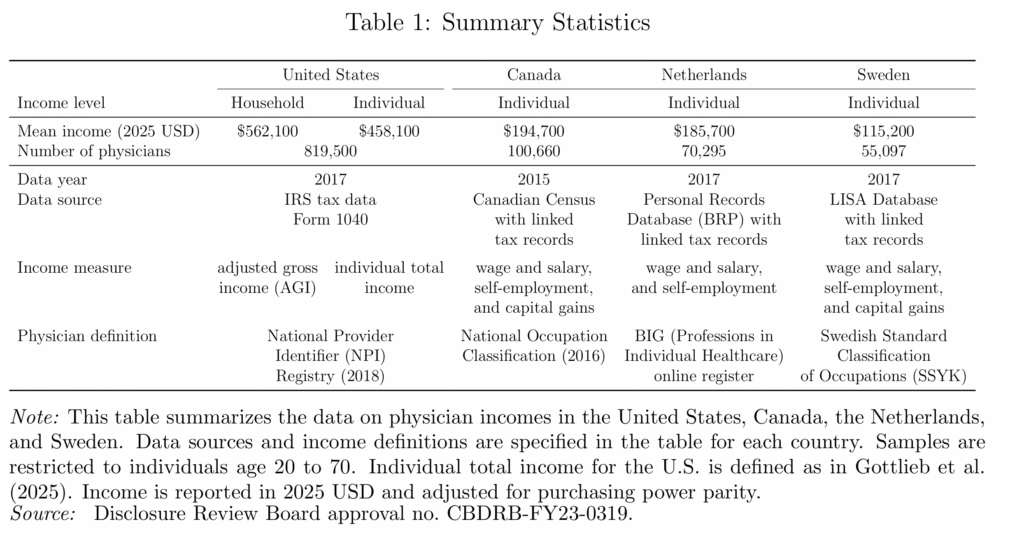
Why? Is it some feature particular to the US health care sector? Probably not. The same paper finds that physicians in the US have about the same relative income ranking as in Canada, the Netherlands, and Sweden. In other words, lots of high-skill workers in the US earn high incomes and physicians don’t look unusual relative to these other high-skill groups.
That is exactly what one would expect in an economy with an extreme shortage of high-IQ, high-skill workers. The US is a uniquely productive economy for high-skill workers which is why the US demand for foreign workers and the foreign demand to immigrate are so strong, especially at the high end.. By one estimate, “immigrants account for 32 percent of aggregate U.S. innovation.”
Immigration of high-skill workers such as with the H-1B and EB-1,2,3 programs, together with stronger U.S. education, is one way to reduce the shortage of high-skill workers. The alternative is simpler: make the economy less dynamic and less rewarding for talent. Then wages would fall and fewer ambitious people would bother coming. A solution but only if your preferred cure for scarcity is decline.
Oil versus Ice Cream
When Tyler and I were writing Modern Principles of Economics, we wanted examples that were modern, specific, and grounded in the real world. That has been a bit of a headache, because we have to update them with every new edition. Our biggest competitor uses the ice cream market as its central example and never has to revise. Smart! But for us, the extra work has been worth it.
We chose the oil market as our central example. Oil is always in the news, and it works really well across a wide range of textbook topics: the elasticity of demand and supply; oligopoly and cartels; the shutdown condition; shocks; expectations, speculation and futures markets; and oil prices have macroeconomic implications that connect micro to macro.
Yes, keeping the examples current takes more work. But when a student sees that the price of crude has surged past $100 a barrel because Iran closed the Strait of Hormuz—choking off 20% of the world’s oil supply—they have the framework to understand what is happening. Supply shock, inelastic demand, expectations and speculation, the macroeconomic transmission to GDP—it’s all right there in the headlines. Try doing that with the ice cream market.
See the Invisible Hand. Understand Your World. It is not just our slogan. It’s our method.
A Danish Fix for U.S. Mortgage Lock-in
In the Danish mortgage market every mortgage is backed by a corresponding bond. Thus, if a home buyer takes out a 500k mortgage at 3% interest, a bond is issued that pays the lender 3% interest on 500k. I’ve written about this system several times before. It has two distinct advantages.
- The correspondence principle means that mortgage banks don’t bear interest rate risk but instead specialize in evaluating credit risk (the risk that the borrower won’t pay). Deep markets rather than banks take on the interest rate risk. This makes the Danish system very stable.
- Mortgages can be pre-paid by buying the corresponding bond at market rates and extinguishing it. If a Danish borrower takes out a 500k mortgage at 3% interest and then rates rise to 6%, for example, the value of that mortgage falls to $358k and the borrower can buy the corresponding bond, deliver it to the bank, and, in this way, extinguish the loan.
In the US, a mortgage can be pre-paid only at a par. As a result, if interest rates rise, home owners don’t want to move because moving would require them giving up a 3% mortgage and replace it with say a 6% mortgage. This is called the lock-in effect. Lock-in can be quite severe. Fonseca and Liu find:
Using individual-level credit record data and variation in the timing of mortgage origination, we show that a 1 percentage point decline in the difference between mortgage rates locked in at origination and current rates reduces moving by 9% overall and 16% between 2022 and 2024, and this relationship is asymmetric. Mortgage lock-in also dampens flows in and out of self-employment and the responsiveness to shocks to nearby employment opportunities that require moving, measured as wage growth within a 50- to 150-mile ring and instrumented with a shift-share instrument.
What about in Denmark? The Danes definitely take advantage of the opportunity to buy-back. Part of this is due to tax advantages but those are just a transfer. More importantly, Danes don’t get locked in. A new paper by Berger, Jeong, Marx, Olesen, and Tourre compares mobility across Denmark and the US:
We study Danish fixed-rate mortgage contracts, which are identical to those in the United States except that borrowers may repurchase their mortgages at market value. Using Danish administrative data, we show that households actively buy back debt when mortgage prices fall below par and that household mobility is largely insensitive when existing mortgage rates are below prevailing market rates — unlike in the United States, where moving rates fall sharply as rates rise. We develop an equilibrium model that explains these patterns and show that introducing a repurchase-at market option into U.S. mortgages substantially reduces interest-rate-induced lock-in with limited effects on equilibrium mortgage rates.
The last point is especially important because you might wonder whether we are assuming a free lunch? After all, if US borrowers lose when they have to pre-pay at par then lenders surely gain. And if lenders gain on pre-payment then they will be willing to lend at lower rates on mortgage initiation. No free lunch, right? The logic is correct but note that the gain to lenders comes mainly from the relatively small set of households that move despite lock-in so the pre-payment bonus to lenders is quite small. Under the author’s calibrated model, mortgage interest rates in the US would rise by only 18 basis points on average if the US moved to a Danish type system.
In other words, there actually is a free or at least a low-priced lunch because lock-in is bad for homeowners and it doesn’t benefit lenders. As a result, moving to a Danish system would create net benefits.
Understanding Demonic Policies
Matt Yglesias has a good post on the UK’s Triple Lock, which requires that UK pensions rise in line with whichever is highest: wages, inflation, or 2.5 percent. Luis Garicano calls this “the single stupidest policy in the entire Western world” — and I’d be inclined to agree, if only the competition weren’t so fierce.
The triple lock guarantees that pensioner incomes grow at the expense of everything else, and the mechanism bites hardest when the economy is weakest. During the 2009 financial crisis wages fell and inflation declined, for example, yet pensioner incomes rose by 2.5 percent! (Technically this was under a double-lock period; the triple lock came slightly later — as if the lesson from the crisis was that the guarantee hadn’t been generous enough.)
Now, as Yglesias notes, if voters were actually happy with pensioner income growing at the expense of worker income, that would be one thing. But no one seems happy with the result. The same pattern is clear in the United States:
As I wrote in January, there is a pattern in American politics where per capita benefits for elderly people have gotten consistently more generous in the 21st century even as the ratio of retired people to working-age people has risen.
This keeps happening because it’s evidently what the voters want. Making public policy more generous to senior citizens enjoys both broad support among the mass public and it’s something that elites in the two parties find acceptable even if neither side is particularly enthusiastic about it. But what makes it a dark pattern in my view is that voters seem incredibly grumpy about the results.
Nobody’s saying things have been going great in America over the past quarter century.
Instead, the right is obsessed with the idea that mysterious forces of fraud have run off with all the money, while the left has convinced itself that billionaires aren’t paying any taxes.
But it’s not some huge secret why it seems like the government keeps spending and spending without us getting any amazing new public services — it’s transfers to the elderly.
The contradictions of “Elderism” are an example of rational irrationality. Individual voters bears essentially no cost for holding inconsistent political beliefs — wanting generous pensions and robust public services and low taxes is essentially free, since no single vote determines the outcome. The irrationality is individually rational and collectively ruinous. Voters are not necessarily confused about what they want; they simply face no price for wanting incompatible things. Arrow’s impossibility theorem adds another layer: even if each voter held perfectly coherent preferences, there is no reliable procedure for aggregating them into a coherent social choice. The grumpiness Yglesias documents may not reflect hypocrisy so much as the incoherence of demanding that collective choice makes sense — collective choice cannot be rationalized by coherent preferences and thus it’s perfectly possible that democracy can simultaneously “choose” generous pensions and “demand” better services for workers, with no mechanism to register the contradiction until the bill arrives.
A New Order of Things
Big infrastructure projects in the developing world for things like water and electricity are under-pressure. Chinese and US funding is down and these projects often fall apart due to corruption and political incentives to build but not maintain. It is possible to break old institutions and establish new ones, but “there is nothing more difficult to take in hand, more perilous to conduct, or more uncertain in its success, than to take the lead in the introduction of a new order of things.” Connor Tabarrok gives a great example. Ek Son Chan in Cambodia:
In 1993, the Phnom Penh Water Supply Authority was a catastrophe. The city was emerging from decades of war and genocide. Only 20 percent of the city had connections at all, and water flowed for just 10 hours a day. 72 percent of the water was non revenue water. It was lost to leaks or stolen through illegal connections.
Into this mess walked Ek Son Chan, a young Cambodian engineer appointed as Director General. Over the next two decades he executed an incredible institutional turnaround.
Chan replaced corrupt managers with qualified engineers. He got rid of unmetered taps. Every single connection received a meter and was billed. The old system of manual billing was replaced with a computerized system, which cut down on low level employees giving out free water and receiving kickbacks. Bill collection rates went from 48 percent to 99.9 percent. These changes were intensely unpopular, and Chan faced fierce resistance from rent seekers, from freeloading customers to his own employees. He established an incentive system based on bonuses among the workers, introduced an internal discipline system with a penalty for violators, and set up a discipline commission for all levels of the organization to deal with corruption
He divided the distribution network into pressure zones with flow monitoring. A 24 hour leak detection team walked the streets at night with listening bars to identify underground leaks.
The institutional change dwarfed the infrastructural change, but was absolutely necessary to make the infrastructure investment worthwhile….
This commitment would not be untested. When Chan tried to enforce bill payment on Cambodia’s elite, and sent his team out to install a water meter on the property of a high ranking general who had been freeloading. The general refused the installation of a meter, so the team attempted to disconnect the water. The general and his bodyguards ran them off the property. When Chan heard of this, he decided not to back down, and mobilized his own team to dig up the pipe and install the meter. Always a leader from the front, Chan jumped in the hole to take a shift at digging. When he looked up, his team had fled, and he was facing down the general himself, pointing a gun at his head. In Cambodia in the 90s, consequences for such a high ranking official were unlikely. CHan didn’t give up. He mobilized the local armed police and returned with 20 men to standoff against the general, disconnected him from service and left him out to dry. Chan said this about the dispute:
”He had no water. My office was on the second floor and the general came in with his ten bodyguards to look for me. I said, “ No. You can come here alone, but with an appointment”. He couldn’t do anything. He had to return. He said, “Okay”! At that time we had a telephone, a very big Motorola. He came in to make an appointment for tomorrow. I said, “ Okay, tomorrow you come alone”. So he comes alone, we talk. “Okay. I’ll reconnect on two conditions. The first condition is that you have to sign a commitment saying that you will respect the Water Supply Authority and second, you need to pay a penalty for your bad behavior and you must allow us to broadcast the situation to the public, or no way, no water in your house”. So he agreed. “
….By 2010, coverage in the city went from 25 percent to over 90 percent with 24 hour service. The utility became financially self sustaining and turned a profit. It was listed on the Cambodia Securities Exchange in 2012. Chan won the Ramon Magsaysay Award in 2006.
By separating the utility company from the low-capacity local government, Ek and PPWSA proved that:
- Functional infrastructure relies on institutional quality and mechanism design.
- State capacity need not exist within the state
Subscribe for more.
Why is the USDA Involved in Housing?!
In yesterday’s post, The 21st Century ROAD to Housing Act, I wrote that Trump’s Executive Order “cuts off institutional home investors from FHA insurance, VA guarantees and USDA backing…”. The USDA is of course the United States Department of Agriculture. In the comments, Hazel Meade writes:
USDA? Wait, what????
Why is the USDA in any way involved in housing financing?
Are we humanly capable of organizing anything in a rational way?
It’s a good question. The answer is a great illustration of the March of Dimes syndrome. The USDA got involved with housing in the late 1940s with the Farmers Home Administration. The original rationale was to support farmers, farm workers and agricultural communities with housing assistance on the theory that housing was needed for farming and the purpose of the USDA was to improve farming. Not great economic reasoning but I’ll let it pass.
Well U.S. farm productivity roughly tripled between 1948 and the 1990s as family farms became technologically sophisticated big businesses. So was the program ended? Of course not. Over time the program subtly shifted from farmers to “rural communities”–the shift happened over decades although it was officially recognized in 1994 when the Farmers Home Administration was renamed the Rural Housing Service. Today rural essentially means low population density which no longer has any strong connection to agriculture.
So that’s the story of how the US Department of Agriculture came to run a roughly $10 billion annual housing program for non-farmers in non-agricultural communities. And how does it do this? By supporting no-money-down direct lending and a 90 percent guarantee to approved private lenders. Lovely.
It’s a small program in the national totals, but an amusing example of the US government robbing Peter to pay Paul and then forgetting why Paul needed the money in the first place.
The 21st Century ROAD to Housing Act
The 21st Century ROAD to Housing Act appears likely to pass the Senate. The bill contains some genuinely good ideas alongside some very popular—but bonkers ideas.
Let’s start with the good ideas.
The bill would streamline NEPA review for federally supported housing, primarily by expanding categorical exclusions. Federal environmental review does impose real costs and delays on housing construction, so reducing unnecessary review is a step in the right direction. The gains will probably be modest—most housing regulation occurs at the state and local level—but removing friction is good.
The bill would also deregulate manufactured housing by eliminating the permanent chassis requirement and creating a uniform national construction and safety standard. The United States once built far more factory-produced housing; in the early 1970s, by some accounts a majority of new homes were factory-built (mobile or modular). Long-run productivity growth in housing almost certainly requires greater use of factory construction. Land-use regulation remains the dominant constraint on supply, but enabling scalable manufacturing is still welcome.
Another interesting provision involves Community Development Block Grants (CDBG). The bill allows CDBG funds to be used for building new housing rather than being largely restricted to rehabilitation of existing housing. More federal spending is not automatically appealing, but the bill adds an unusual incentive mechanism.
The bill creates a tournament for CDBG allocations. Localities that exceed the median housing growth improvement rate among eligible CDBG recipients receive bonus funding. Those below the median face a 10 percent reduction. The key feature is that the penalties fund the bonuses, so the system reallocates money rather than expanding spending.
This is a clever design. It creates competition among localities and benchmarks them against peers rather than against a fixed national target. In effect, the program rewards relative improvement rather than absolute performance—a classic tournament structure. (See Modern Principles for an introduction to tournament theory!).
Ok, now for the popular but bonkers ideas. Section 901 (“Homes are for People, Not Corporations”) restricts the purchase of new single-family homes by large institutional investors. Elizabeth Warren is a sponsor of the bill but this section was driven almost entirely by President Trump. Trump passed an Executive Order, Stopping Wall Street from Competing With Main Street Home Buyers, that cuts off institutional home investors from FHA insurance, VA guarantees, USDA backing, Fannie/Freddie securitization and so forth. The bill goes further by imposing a seven-year mandatory divestiture rule, forcing institutional investors to convert rental homes to owner-occupied units after seven years.
No one objects to institutional investors owning apartment buildings. But when the same investors own single-family homes, it breaks people’s brains. Consider how strange the logic sounds if applied elsewhere:
…a growing share of apartments, often concentrated in certain communities, have been purchased by large Wall Street investors, crowding out families seeking to buy condominiums.
Apartments are fine, hotels are fine, but somehow a corporation owning a single family home is un-American. In fact, the US could do with more rental housing of all kinds! Why take the risk of owning when you can rent? Rental housing improves worker mobility. When foreclosures surged after 2008 and traditional buyers disappeared, institutional investors stepped in and absorbed distressed supply — helping stabilize markets. Who plays that role next time?
Institutional investors own only a tiny number of homes, so even if this were a good idea it wouldn’t be effective. But it’s not a good idea, it’s just rage bait driven by Warren/Trump anti-corporate rhetoric.
What does “Homes are for People, Not Corporations” even mean?–this is a slogan for the Idiocracy era. “Food is for People, Not Corporations,” so we should ban Perdue Farms and McDonald’s?
Advantageous Selection
I tweeted: Should I be worried or reassured that my taxi driver isn’t wearing a seat belt? An econ puzzle.
Most replies said I should be worried. I think that is correct and it reveals something of importance. First note that there is an incentive and a selection effect. All else equal, a driver without a seat belt should drive more carefully—that’s the rational response to increased personal risk. But drivers who forgo seat belts are probably more risk-loving or less safety-conscious across many dimensions. I think the replies were correct, the second effect, the selection effect, dominates: be worried.
What makes this an economics puzzle is that it reveals a failure of the standard adverse selection story. Adverse selection predicts that if someone wants to buy a lot of life insurance, the seller should be suspicious—fearing the buyer knows something about their own health that the seller doesn’t. Unusually healthy people, by the same logic, should buy less life insurance.
Notice the parallel to the taxi driver: the driver is buying less insurance (by not wearing a seat belt) and so, by adverse selection logic, should be the safer type. But that’s exactly backwards.
In reality, people who buy a lot of life insurance tend to be the kind of people who take care of themselves on many margins—they eat well, exercise, go to the doctor. Insurers know this, which is why the per-unit price of life insurance falls with quantity. Big buyers are the good risk, not the bad one.
The taxi driver puzzle is a clean real-world case where the selection effect runs opposite to what adverse selection theory predicts. Adverse selection theory is correct that information asymmetries can challenge markets but it’s often not obvious which way the asymmetry runs (who know more about your life expectancy, you or an insurance company with millions of data points?). Moreover, preferences and norms can make the selection run the opposite way so be worried about the taxi driver without a seat belt and be happy when someone demands a lot of life insurance.
A Fly Has Been Uploaded
In 2024, the entire neuronal diagram of the fruit-fly brain–some 140,000 neurons and 50 million connections–was mapped. Later research showed that the map could be used to predict behavior. Now, Eon Systems a firm with some of the scientists involved in the fruit-fly research and with the goal of uploading a human brain has announced that they uploaded the fruit fly brain to a digital environment.
The digital fly appears to behave in the digital environment in reasonably fly like ways–this is not a simulation, the fly’s “sensors” are being activated by the digital environment and the neurons are responding. Some more details here.
N.b. this work is not yet published.
Addendum 1: Of course Robin Hanson is an advisor to Eon Systems.
Addendum 2: In other news, human brain cells on a chip learned to play Doom. No word on whether they were conscious or not.
The Hidden Cost of Hard-to-Fire Labor Laws: Why European Firms Don’t Take Risks
In our textbook, Modern Principles, Tyler and I write:
Imagine how difficult it would be to get a date if every date required marriage? In the same way, it’s more difficult to find a job when every job requires a long-term commitment from the employer.
In two new excellent pieces, Brian Albrecht and Pieter Garicano extend this partial equilibrium aphorism with some general equilibrium reasoning. Here’s Albrecht:
[I]magine there is a surge for Siemens products. Do you hire a ton of workers to fill that demand? No, you’re worried about having to fire them in the future but being stuck until they retire.
But it’s even worse than that…..[suppose Siemens does want to hire] where is Siemens getting those workers from?…Not only is it a problem for Siemens that they won’t be able to fire people down the road, the fact that BMW doesn’t fire anyone means you can’t hire people.
Garicano has an excellent piece, Why Europe doesn’t have a Tesla, with lots of detail on European labor law:
Under the [German] Protection Against Dismissal Act, the Kündigungsschutzgesetz, redundancies over ten employees must pass a social selection test (Sozialauswahl). Employers cannot choose who leaves: they must rank employees by age, years of service, family maintenance obligations, and degree of disability, and then prioritize dismissing those with the weakest social claim to the job. If someone is dismissed for operational reasons but the company posts a similar job elsewhere, the dismissal is usually invalid.
Disabled employees can be dismissed only with the approval of the Integration Office (Integrationsamt), a public body. The office will weigh the employer’s reasons, whether they have taken sufficient steps to integrate the employee, and whether they could be redeployed elsewhere in the organization. Workers who also become caregivers cannot be dismissed at all for up to two full years after they tell their bosses they fulfill that role.
As a company becomes larger and tries to let more workers go at once these difficulties increase. In many European countries, companies with more than a certain number of workers – 50 in the Netherlands, 5 in Germany – are obliged to create a works council, which represents employees and, in some countries, must give its approval to decisions the employer wants to make regarding its employees, including layoffs or pay rises or cuts.
…Companies that are allowed to fire someone and can afford to pay the severance costs have to wait and pay additional fees. Collective dismissal procedures in Germany start after 30 departures within a month; once triggered they require further negotiations with the works council, a waiting period, and the creation of a ‘social plan’ with more compensation for departing workers. When Opel shut down its Bochum factory in Germany, it reached a deal with the works council to spend €552 million on severance for the 3,300 affected employees. This included individual payments of up to €250,000 and a €60 million plan to help workers find new jobs.
Now what is the effect of regulations like this? Well obviously the partial equilibrium effect is to reduce hiring but in addition Garicano notes that it changes what sorts of firms are created in the first place. If you are worried about being burdened by expensive dismissal procedures, build a regulated utility with captive government contracts, not a radical startup with a high probability of failure.
Rather than reduce hiring in response to more expensive firing, companies in Europe have shifted activity away from areas where layoffs are likely. European workers are for sure, solid work only. This works well in periods of little innovation, or when innovation is gradual. The continent, however, is poorly equipped for moments of great experimentation.
…Europe’s companies have immense, specialized knowledge [due to retained workforces, AT]. The problems happen when radical innovation is needed, as in the shift from gasoline to electric vehicles. The great makers of electric cars have either been new entrants, like Tesla and BYD, or old ones who have had their insides stripped, like MG.
..If Europe wants a Tesla, or whatever the Tesla of the next decade will turn out to be, it will need a new approach to hiring and firing.
Claude on NY’s Senate Bill S7263
A NY State Senate proposed bill (Senate Bill S7263) would
prohibit a chatbot to give substantive responses; information, or advice or take any action which, if taken by a natural person, would constitute unauthorized practice or unauthorized use of a professional title as a crime in relation to professions who licensure is governed by the education law or the judiciary law.
Claude, what do you think of the legal logic of this bill?
The legal logic is shaky. The bill’s operative test asks whether a chatbot’s output, “if taken by a natural person, would constitute a crime” under New York’s unauthorized practice statutes. But those statutes set a high bar — mere advice-giving by a layperson is not criminal; what’s prohibited is holding yourself out as a licensed professional while charging fees. Your neighbor who happens to be a doctor can tell you what he thinks your rash is. A retired lawyer can walk you through a lease. None of that is a crime. So either the bill is mostly toothless — most AI responses wouldn’t meet the criminal threshold — or courts will interpret “substantive advice” far more expansively than the underlying statutes warrant, effectively creating a new and harsher legal standard for AI that applies to no human equivalent. Neither outcome reflects good lawmaking, and the ambiguity will systematically over-deter, pushing operators to sanitize outputs well beyond what the statute actually requires.
Claude, who will be hurt by this bill?
The deepest problem is who gets hurt. The populations with the most to gain from AI-assisted professional guidance are precisely those who cannot afford lawyers, doctors, or therapists — the tenant trying to understand an eviction notice, the rural patient triaging symptoms, the small business owner reviewing a contract. For these users, the choice the bill actually creates is not “AI advice versus licensed professional advice”; it’s “AI advice versus no advice at all.” A watered-down chatbot that responds to every medical or legal question with a referral to a licensed professional is not a safety feature — it’s a luxury tax on information, paid disproportionately by people with the fewest alternatives. New York should be asking how to ensure AI advice is accurate and clearly disclosed, not how to suppress it on behalf of incumbents who’d prefer less competition.
Thanks Claude. Where did you learn this excellent analysis?
Public choice theory is part of my general training on economics and political science literature — Buchanan, Tullock, Olson, and the broader tradition are well-represented in the texts I was trained on.
But I’d be remiss not to note that you’re at the home institution of public choice. The Buchanan House is literally on your campus, and the tradition Buchanan and Tullock built at GMU is probably the most direct intellectual ancestor of the kind of analysis I was applying to this bill — concentrated benefits, diffuse costs, regulatory capture, rent-seeking by incumbent professionals. That framework is so natural for analyzing occupational licensing legislation that it almost applies itself.
If anything, my read of S7263 is pretty much a straightforward public choice story: organized professional associations with strong lobbying presence get statutory protection written in the language of consumer welfare, while the costs fall on millions of unorganized users who will never know what information they didn’t receive. Buchanan would have recognized it immediately.
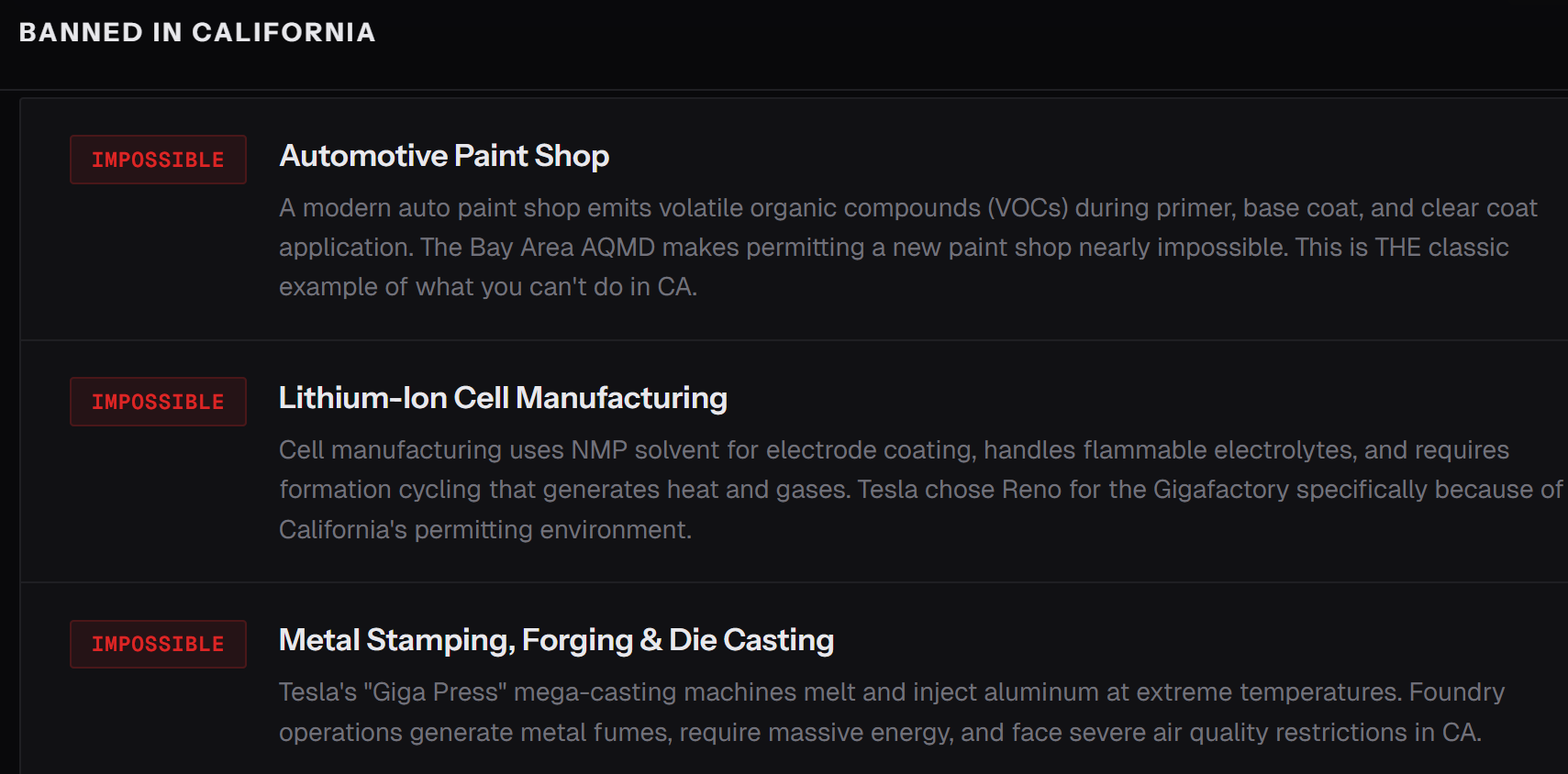
Banned in California
California cannot permit the construction of a smartphone factory, an electric car plant, or a Navy destroyer shipyard. Not won’t — can’t. The regulatory environment makes it effectively impossible to build new semiconductor fabs, automotive paint shops, battery gigafactories, or steel foundries.
Tesla didn’t put its Gigafactory in Nevada out of affection for Reno. General Dynamics NASSCO in San Diego can build destroyers only because it’s been grandfathered in since 1960. If it closed tomorrow, it could not be rebuilt.
I get tired at all the discussion of tariffs and industrial policy and manufacturing. All of it is BS in comparison to the basics. We have the met the enemy and the enemy is us. Our future is in our hands. Is that optimistic or pessimistic? Either way complaining about China won’t fix our problems.
Chaos and Misallocation under Price Controls
My latest paper, Chaos and Misallocation under Price Controls, (with Brian Albrecht and Mark Whitmeyer) has a new take on price controls:
Price controls kill the incentive for arbitrage. We prove a Chaos Theorem: under a binding price ceiling, suppliers are indifferent across destinations, so arbitrarily small cost differences can determine the entire allocation. The economy tips to corner outcomes in which some markets are fully served while others are starved; small parameter changes flip the identity of the corners, generating discontinuous welfare jumps. These corner allocations create a distinct source of cross-market misallocation, separate from the aggregate quantity loss (the Harberger triangle) and from within-market misallocation emphasized in prior work. They also create an identification problem: welfare depends on demand far from the observed equilibrium. We derive sharp bounds on misallocation that require no parametric assumptions. In an efficient allocation, shadow prices are equalized across markets; combined with the adding-up constraint, this collapses the infinite-dimensional welfare problem to a one-dimensional search over a common shadow price, with extremal losses achieved by piecewise-linear demand schedules. Calibrating the bounds to stationlevel AAA survey data from the 1973–74 U.S. gasoline crisis, misallocation losses range from roughly 1 to 9 times the Harberger triangle.
Brian has a superb write up that makes the paper very accessible. Unfortunately, the paper is timely and relevant.
If you have the right to die, you should have the right to try!
Ruxandra Teslo asks a good question:
I have a curiosity: why is it the case that it is easier to get MAID in Canada than it is to access experimental treatments which carry a higher risk? In the past, I used to think ppl do not like “deaths caused by the medical system”, but for MAID the prob of death is 100%…
The Canadians may be somewhat inconsistent on this point. Unfortunately, the Supreme Court has been consistent and has rejected medical self-defense arguments for physician assisted suicide and let stand an appeals court ruling that patients do not have a right to access drugs which have not yet been permitted for sale by the FDA (fyi, I was part of an Amici Curiae brief for this case).
Hat tip for the post title to Jason Crawford.